AADD-UK
Advocacy
Bristol Adult ADHD Service Update
Monday, 31 July 2023:
This is just a quick update to say that this project is still ongoing, at pace, as is our partnership with the NHS Bristol, North Somerset and South Gloucestershire Integrated Care Board (BNSSG ICB) and Avon and Wiltshire Mental Health Partnership NHS Trust (AWP) and we are making progress. As we stated before, it is a multi-layered and complex project, it will take time to complete, but please be assured all three partners are fully committed and are working hard.
Thursday, 18 August 2022:
We wholeheartedly apologise for the long delay in updating this post but we have been working hard for some time now, and good news, we have established a relationship of trust and partnership with the NHS Bristol, North Somerset and South Gloucestershire Integrated Care Board (BNSSG ICB) formerly known as NHS BNSSG Clinical Commissioning Group, as well as with the Avon and Wiltshire Mental Health Partnership NHS Trust (AWP).
The three partners, representatives of the Bristol Adult ADHD Support Group & AADD-UK, BNSSG ICB, and AWP are working jointly and collaboratively, at pace, on designing and piloting an Adult ADHD Service that will be cost effective (now and in the future), that will effectively and efficiently integrate care. The service will be high quality, safe and it will give service users a positive experience. All service users will receive integrated care.
All three partners are fully committed to the project, but since it is multi-layered and complex it will take some time to complete. We have, however, made good progress and where we can, we will be making some improvements along the way. We are particularly concerned with the waiting list.
We will provide project updates here from time to time, but please do not worry if you don’t hear anything, it simply means we are working very hard on this exciting and positive project.
We are now putting a line between this post and the old posts below.
By way of background, on 6 December 2019, two years and two months ago, the Bristol Adult ADHD Support Group filed their first formal NHS complaint with Bristol North Somerset South Gloucestershire Clinical Commissioning Group (BNSSG CCG) regarding the very long waiting list. As a result of that complaint, in June 2020 a joint working group was formed with BNSSG CCG, AWP, and the Bristol Adult ADHD Support Group to address the waiting list matter and to develop a sustainable and effective adult ADHD service model. Everyone worked hard for the next six months until January 2021 when the project was paused by the CCG citing heavy Covid-19 work loads. After several unsuccessful attempts to get the project restarted, the Bristol Adult ADHD Support Group on Monday, 13 December 2021, filed a second formal NHS Complaint titled, Failure to fulfill resolution to complaint of 6 Dec 2019. The CCG replied with a commitment to continuing the work and the support group is currently waiting, yet again, for meeting dates.
For details, please read the timeline below (to read in date order, scroll to the bottom and read upwards):
Monday, 21 February 2022
On 17 January 2022, in response to the CCG’s assurance that they were committed to restarting the ADHD project, the Bristol Adult ADHD Support Group sent an email to the CCG in which the group listed the dates they were available for meetings. The CCG’s reply to this email has been silence, nothing! So, today the Bristol Adult ADHD Support Group sent the following email to the CCG:
RE: 2834 NHS Formal Complaint – Remaining concerns and outcomes/commitments & Potential Additional Complaints
Dear [Customer Service Manager],
Could you please ensure that this email is also forwarded to xxxx xxxxxx, CCG CEO.
Since it has now been more than one year when service user participation in the joint collaborative adult ADHD working group project was paused, I would appreciate it if you could, please, contact the investigator/relevant parties at the CCG and check that they are still on track with following up on my letter of Remaining Concerns dated 25 January 2022.
I wish to avoid slippage in the timeframe that you gave me in your email of 27 January, particularly since promises given by xxxxxx xxxxxx regarding other matters have already been broken as I detail in the following paragraphs.
I am extremely disappointed that despite assurances from xxxxx xxxxxx in her complaint response of 14 January 2022 that I would be contacted by both xxxxxxx xxxxxxx and xxxxxxx xxxxxxx, this has not happened – even with (in the case of xxxxxx) my having sent my meeting availability on 17 January 2022 as confirmed by your email of 18 January.
I had already raised the matter of my emails being met with either silence or vague promises of dates which never materialised in the fourth paragraph of my formal complaint letter of 13 December 2021, and again as the third concern in my letter regarding ‘Remaining Concerns’ of 25 January 2022.
The lack of contact from both xxxxx xxxxxx and xxxxxxx, is therefore another “concern”, and I would like it to be rectified to my satisfaction by end of day on Wednesday, 2 March 2022.
If this does not happen, I would like this to be added as “additional complaints” and responded to in the CCG’s further response when it is issued.
Under the terms of The Local Authority Social Services and National Health Service Complaints (England) Regulations 2009, such silence and failure to follow through could be viewed as neither treating me “with respect and courtesy” (per Reg 3(2)(c)) nor resolving my complaint with needed remedial action “speedily and efficiently” (Regulation 14(1)(a) and Regulation 3(2)(a)) contrary to Julia Ross’s promises. In short it is also therefore poor complaints handling.”
Kind regards,
Tuesday, 25 January 2022
The Bristol Adult ADHD Support Group sent a letter, NHS Formal Complaint – Remaining concerns and outcomes/commitments, to the CCG as a follow-up on their response thus,
I am in general pleased to read in your response letter of 14 January that the CCG is ‘happy to meet to reset the position and to continue the working group’, and that xxxx xxxxxx will be in contact to plan specific dates. On 17 January I sent my availability for meeting dates to the CCG and received confirmation the next day that this has been shared with the team.
However, I also have four remaining concerns and outcomes/commitments that I am seeking as follows:
1. Variations in the frequency of our meetings should be jointly agreed between all three partners of the working group (the CCG, AWP, and service users) per our Terms of Reference, and except in cases of emergencies, these variations should be planned. We are reasonable people and understand Covid-19 constraints and pressures.
2. Decisions to cancel or postpone meetings should not be unilaterally taken by any one partner of the working group. These decisions should be jointly agreed by all three parties and at the same time we should agree the date of the next meeting. In other words, the cancellation or postponement will be of limited duration, and we will all know when to expect the next meeting. And except in cases of emergency, cancellations and postponements should be planned. We should also investigate amending our Terms of Reference at our forthcoming meeting to include cancellations and postponements.
3. Follow-on meeting dates should be agreed at the end of each meeting, if not sooner, and should be regarded as firm commitments. We, service users, do not want to go through another seven months of sending chasing emails and receiving only silence or vague promises that never materialise as described in my letter of 13 December 2021.
4. I would also like to receive copies of any ADHD related documents that were produced during the time that our, service user, involvement was paused (from December 2019 to present) so that we can bring ourselves up to date. For example, I understand that meetings were held regarding ADHD provision within the CCG and between the CCG and AWP that the CCG failed to invite the ADHD service user group to
as seen in the three attached examples from the CCG’s May 2021 draft Target Operating Model for BNSSG Integrated Community Mental Health Service (Adults), the Quality Control Committee minutes for July 2021, and the Corporate Risk Register for December 2021 (with regard to the latter, contrary to what is stated in the note for Aug 21, we only had a holding invite to a meeting on 2 September 2021 which was subsequently cancelled). Other examples can be found in the public Governing Body meeting papers from April 2021 until present.
I am looking forward to hearing very soon from xxxxx xxxx so that we can plan specific dates for resuming our work. And I am also looking forward to hearing soon from xxxxx xxxxxx so that people with ADHD can be involved in the development of Community Mental Health Services and Integrated Care Partnerships.
However, I would like to receive a written response from you to my outstanding concerns including confirmation that you are in agreement with the remaining outcomes/commitments I am seeking and look forward to hearing from you as soon as possible.
Monday, 17 January 2022
The Bristol Adult ADHD Support Group sent an email to the CCG in reply thanking them and sending their availability dates.
Friday, 14 January 2022
BNSSG CCG replied to the support group’s complaint with some good news. Here are two extracts from their letter:
. . .
Like you, I am personally disappointed that we have not yet been able to deliver the improvement needed along with key recommendations made by the working group, that we have previously discussed at our Clinical Executive meeting. I know that Avon and Wiltshire Mental Health Partnership (AWP) were keen to respond to the recommendations and using the additional investment that was made available to
support recruitment. However, to date this has not been possible. I do appreciate that there have been many delays to getting meetings in the diary which will have been frustrating for you, and for that I apologise. I have discussed with the team the need to improve communication and ensure that they are clearer in future.
. . .
In summary and in relation to the outcomes you have requested. We are happy to meet to reset the position and to continue the working group. xxxx xxxxx will be in touch to get specific dates planned. We may need to consider how frequently the group meets to ensure that we set realistic expectations for all, given the current circumstances. I hope this will enable us to start the year with renewed positive focus on this important agenda and make critical changes in partnership with all our providers and the people we serve, to shape the better outcomes for people with ADHD.
Monday, 13 December 2021
The Bristol Adult ADHD Support Group sent their second formal NHS Complaint letter (with eight supporting documents) to the CCG. Their letter is six pages long so we have only included extracts here:
I filed my first formal NHS complaint, Serious concerns about BNSSG’s handling of the Adult ADHD Service waiting list, on 6 December 2019 (a copy is attached). On 28 April 2020, representatives from the CCG, Avon and Wiltshire Mental Health Partnership NHS Trust (AWP), and myself and two other service user representatives attended a Local Resolution Meeting (LRM) at which we all agreed to form a Joint Collaborative ADHD Working Group project which had both a short-term objective (reduction of the waiting list) and a long-term objective (an effective and sustainable adult ADHD service). Terms of Reference (ToR) were agreed on 30 June 2020 (a copy is attached).
Since the short-term objective (finding and implementing solutions for the current waiting list) was urgent, this became our focus for six months although we did manage to fit in some work on the long- term objective. But we had not completed the short-term objective (due to interrelated complexities) and we had only completed about of third of the work needed for the long-term objective when the CCG, citing Covid-19 work pressures, sent an email to the joint ADHD working group on 2 February 2021 in which they, understandably at the time, explained, they had ‘taken the decision to stand down our meeting scheduled for this Friday (5th Feb), which will be rescheduled to March 2021’ (a copy is attached).
March passed without us hearing anything from the CCG, so I sent an email to them on 6 April 2021 asking if the pressure had eased enough that we could start considering dates for resuming our work. I sent a follow-up email on 21 April. I sent further emails on 12 July, 11 August, 27 August, 1 September, and 6 October 2021. In these emails I not only asked for future meeting dates, I also reminded the CCG of our agreed resolution and our terms of reference. In the later emails, I pointed out that some of the Governing Body meeting documents seemed to imply the CCG and AWP were working together on ADHD related matters during the time the joint collaborative working group was paused, which, if correctly reported, would not only be contrary to our terms of reference and our agreed resolution, it meant service user insight and perspective was being ignored. We were excluded.
Additionally, I spelt out various service user concerns: high distress levels, growing waiting lists, unhappiness with a provider’s performance, Right to Choose errors, potential impact of upcoming legislative changes upon service provision (Integrated Care Systems); as well as the ever-expanding passage of time since the joint ADHD working group last met in December 2019. From April 2021 until October, my emails either met with silence or vague promises of future meeting dates which never materialised.
. . .
On Friday, 29 October, the CCG replied to say they could not provide a ‘formal written response’ (I had actually asked for a written commitment which is different from a response). Instead, they invited me (and only me) to a meeting to discuss my concerns and ‘talk through next steps together’. This was very disappointing because the CCG not only seemed to have forgotten that our Terms of Reference required us to work collaboratively (which meant I could not agree next steps without involvement of all the other members), but also the invitation contained no guarantee whatsoever that our involvement would resume. There was no commitment from the CCG.
The CCG does admit, however, that the ADHD is unfinished, ‘[w]e have been talking at our Exec to Exec meeting this week between AWP and the CCG about the issues and the challenges we still need to address for people with ADHD’. Which raises questions as to how and what they were discussing since the joint collaborative working group seemingly had not met for 10 months. We had not been involved for the last 10 months. We had been excluded.
The CCG’s response, therefore, also raised the possibility that they had slipped into tokenistic service user involvement. As the transcript for our presentation at the Local Resolution Meeting held on 28 April 2020 shows, the outcome we wanted to achieve from our complaint was a multi-partner and collaborative working group which ‘must be a proper collaborative working group without tokenism’.
It seems the CCG has forgotten, or lost focus on, the reasons for forming the joint ADHD working group; has forgotten, or lost focus on, the supporting Terms of Reference; has forgotten, or lost focus on, the importance of our long-term objective of having an effective and sustainable Adult ADHD Service. It seems, the ADHD project has been deprioritised. It seems the CCG does not understand the very serious impact this has on the lives of service users. I felt, with sadness and disappointment, that I was left with no choice but to file this formal NHS complaint.
Impacts on service users.
The Bristol NHS ADHD Clinic had a growing waiting list before the COVID-19 pandemic arrived (three people on the waiting list killed themselves in 2018). There were two alternative providers under Right to Choose terms. But one of them has now got a one year waiting list, and the other has been rated by the Care Quality Commission as ‘Requires improvement’ overall and specifically in the areas of safety and leadership. This means those service users within the BNSSG area who cannot pay for private ADHD assessments, do not have access to timely and safe NHS ADHD services. This is now a matter of serious health inequality.
People with ADHD are at increased risk for obesity, asthma, allergies, diabetes mellitus, hypertension, sleep problems, psoriasis, epilepsy, sexually transmitted infections, abnormalities of the eye, immune disorders, and metabolic disorders. They are also at increased risk for low quality of life, substance use disorders, accidental injuries, educational underachievement, unemployment, gambling, teenage pregnancy, difficulties socializing, delinquency, suicide, and premature death (Faraone et al., 2021).
I made the case in joint working group meetings that investing in ADHD services is beneficial because it helps offset substantial costs in other parts of the healthcare system as well as in other societal sectors. I produced and disseminated an annotated bibliography that supported my case (a copy is attached with this letter).
. . .
At the Local Resolution Meeting for my first complaint (28 April 2020) we presented a compilation of people’s experiences living with ADHD which had been submitted by members of the Bristol Adult ADHD support group. This narrative clearly showed that many people with undiagnosed ADHD live with very high levels of stress and distress and that their lives are precariously balanced between coping and not coping, and some have experienced significant mental health breakdowns requiring hospitalisation. The narrative also showed that those who had been through the Bristol NHS Adult ADHD Clinic valued the service and staff very highly (a copy of this narrative is attached).
Impact of Covid-19 on people with ADHD
Sadly, many of the people I know in the ADHD community, including other support group leaders, have caught Covid-19, some have been quite ill, and some have had to be hospitalised. The consensus statement, Failure of Healthcare Provision for Attention-Deficit/Hyperactivity Disorder in the United Kingdom (a copy is attached), which I shared with the CCG, warned that that people with ADHD is a group that could be at risk in the pandemic. Here is a relevant extract:
The pandemic is associated with a range of social, financial, educational, health, and personal concerns, which are all stressors associated with mental health issues. Individuals with ADHD are likely to be particularly vulnerable to the distress caused by the pandemic and physical distancing measures, and may display increased behavioral responses. They may also be at greater risk of contracting COVID-19, a risk that appears to be exacerbated in ADHD patients who are untreated. Although these additional pressures on services have arisen more recently and are likely to increase with the exacerbation of clinical needs in this population, they have compounded already existing shortfalls (Young et al., 2021).
. . .
BNSSG’s Corporate Risk Register
The waiting list for adult ADHD services in AWP has been on the CCG’s Corporate Risk Register (CRR) since 5 April 2019. The current risk rating then red 16. As of 28 September 2021, it was still on the CRR and the current risk score was still red, 16. It had therefore been on the CRR for two years and five months at that point.
On 5 October 2021, Agenda item 9.2, Target Risk Scores and Risk Appetite, was presented to the Governing Body for discussion. In the preamble to this document, the following three sections appear:
How does this reduce Health inequalities:
The CCG has a legal duty to reduce health inequalities. A robust Risk Management Framework will support the CCG to reduce Health Inequalities through the identification of risk and mitigating actions, and the implementation of actions, and through the appropriate reporting of risk to ensure oversight by executive management, the CCG sub committees and the Governing Body.
How does this impact on Equality and diversity
The CCG has a legal duty to reduce inequalities. A robust Risk Management Framework will support the CCG to reduce inequalities through the identification of risk and mitigating actions, and the implementation of actions, and through the appropriate reporting of risk to ensure oversight by executive management, the CCG sub committees and the Governing Body
Patient and Public involvement
The CCG has a legal duty to secure public involvement in the planning, development and consideration of proposals for changes and decisions affecting commissioning arrangements. A robust Risk Management Framework will support the CCG to appropriately engagement [sic] with patients and the public through the identification of risk and mitigating actions, and the implementation of actions, and through the appropriate reporting of risk to ensure oversight by executive management, the CCG sub committees and the Governing Body.
With regards to the first section, health inequalities, NHS England on their web page, Definition of Health Inequalities, says ‘action on health inequalities requires improving the lives of those with the worst health outcomes, fastest’.
. . .
With regards to the second section, equality and diversity, NHS England on their webpage, Action required to tackle health inequalities in latest phase of COVID-19 response and recovery, says it has become ‘increasingly clear that COVID-19 has had ‘a disproportionate impact on many who already face disadvantage and discrimination.’ And the impact ‘has been particularly detrimental’ on people living in areas of high deprivation and with protected characteristics. NHS England also says that a ‘central part of responding to COVID-19 and restoring services must be to increase the scale and pace of NHS action to tackle health inequalities to protect those at greatest risk.’
3. Since service users were already disadvantaged and distressed, before the pandemic, due to the lengthy waiting list for ADHD services, will the CCG now understand that the almost one year pause in our work, has had a ‘disproportionate impact’ upon the health, welfare, and safety of this group of service users? Will the CCG commit to the immediate resumption of our project?
With regards to the third section, Patient and Public involvement (PPI), on 7 September 2021, the Well-Led Review Action Plan, was presented to the Governing Body for discussion. In the second paragraph on page five it’s noted that whilst the PPI Forum was stood down due to Covid-19, the PPI subgroups continued to meet in order to ‘maintain a level of connectivity with the local population.’ In the next sentence, the CCG says it is ‘reinstating the PPIF, which is recognised as being particularly important given the CCG’s strategic agenda over the next 6-12 months.’
Given that the ADHD waiting list has been on the CRR for two years and five months, despite its relevance to health inequalities, and to equality and diversity, it is surprising the CCG did not equally recognise the importance of continuing the work of the ADHD joint collaborative working group. They did not ‘maintain a level of connectivity’ with our section of the local population.
4. Will the CCG now commit to the immediate resumption of our project?
Outcomes
• A virtual Local Resolution Meeting either before the end of this year or within the first two weeks of January 2022.
• The full restart of the joint collaborative working group as soon as possible
In summary, I would very much like to re-establish a good working relationship with BNSSG CCG so that together we can achieve an NHS Adult ADHD service that is cost effective (now and in the future), that effectively and efficiently integrates care, is high quality, safe and gives service users a positive experience. A service we can all be proud of.
I look forward to receiving your acknowledgement of this letter.
Monday, 1 November 2021
The Bristol Adult ADHD Support Group replied to the CCG thus:
Thank you for your reply sent end of day on Friday, 29 October, however, after reading it, I realised with disappointment and sadness, I am left with no choice but to file a second formal NHS complaint.
NB: The following is a hasty and incomplete summary of my reasons for this decision and should not be read as my complete case. I am writing this as a courtesy to let you know that a formal and detailed letter of NHS complaint will be forthcoming as soon as possible:
In your reply, you did not provide the CCG’s firm, written commitment to the joint, multi-party, collaborative ADHD working group (BNSSG CCG, AWP, and service user representatives) as I had requested in my emails of 15th and 26th October.
In fact, you made no reference at all to the joint working group nor indeed to the Terms of Reference (ToR) for the joint working group, as if they were non-existent; they were both agreed and adopted by all three parties on Tuesday, 30th June 2020.
Additionally, you tell me the CCG is talking with AWP about ADHD ‘issues and challenges’ without acknowledging that the paused joint working group meetings (a pause enacted and continued by the CCG citing Covid-19 work pressures) means the results of these AWP talks (as well those of previous discussions) cannot be reported back to the joint working group for service user involvement and review before decisions are made, despite the fact that ‘issues and challenges’ fall well within the remit of the joint working group per the jointly agreed ToR; and despite our right to be involved.
Moreover, you invited me to a meeting, outside of the joint ADHD working group, to discuss my ‘concerns in more detail and talk through next steps together’, but inviting me, and only me, to a meeting outside of the joint working group to discuss my concerns (concerns that should be addressed within the joint working group) that the CCG is working on ADHD matters outside the joint working group whilst the joint working group meetings are paused thereby preventing service user involvement not only serves to further delay the resumption of the joint working group, it also makes me complicit in the delay if I accept your invitation. Furthermore, the invitation did not carry a guarantee that the joint working group meetings would restart after we met.
On a personal note, your invitation put me in the difficult position of deciding which would be worse, potentially being accused of justifying further delay without a guarantee by accepting your invitation or potentially being accused of obstruction by not accepting your invitation. I do not appreciate being put in this position after waiting patiently for ten months and then, reasonably, asking the CCG to commit to resuming the joint working group and abiding by our joint agreement.
I am on a waiting list for an advocate with The Advocacy People, hence the case number in the subject line; they are copied in on this email.
As I stated at the beginning, this is a hasty and incomplete summary of my reasoning and should be read as such. A formal and detailed letter of NHS complaint will be forthcoming as soon as possible.
Friday, 29 October 2021
BNSSG CCG replied to the Bristol Adult ADHD Support Group as follows:
Thank you for getting in touch, and for your patience in recent weeks. Whilst I know you are seeking a formal written response there remain issues that we are trying to address and have not yet been able to resolve. As I know you appreciate the challenges of COVID for our workforce the population and the demands on the NHS remain significant. Therefore we have not been able to deliver all the recovery work that we wish we could.
I understand if you feel you need to reopen a formal complaint and that is of course your prerogative. It is really important to us not to lose the open and positive relationship and the investment of time by all parties that has developed over the last 18 months. We have been talking at our Exec to Exec meeting this week between AWP and the CCG about the issues and the challenges we still need to address for people with ADHD. [We] would really value meeting with you alongside xxx xxxx who is the xxxxxx from AWP. We would like to discuss your concerns in more detail and talk through next steps together. Reflecting the reality of the challenges we are facing and how we can do the best for people. xxxxx and xxxxx are looking at dates but is important to understand your availability too.
I am so sorry for the delay in responding to you and getting this set up, and I look forward to hearing from you so we can get something firm in the diary very soon.
Tuesday, 26 October 2021
BNSSG CCG failed to send a written commitment by the deadline date of Monday 25 October, so the Bristol Adult ADHD Support Group sent the following email to them:
Thank you for your email of Friday, 15th saying you would get back to me with a detailed response as soon as possible.
In my email of Friday, 15th, I gave a deadline for replying with the written commitment by end of Monday, 25th (yesterday). But, I now notice that I omitted to specifically state that the ‘reply’ was to be the ‘firm, written commitment’ which was the message I had intended and had meant to convey.
Since my original deadline may have been somewhat confusing, and for that I apologise, I am extending the deadline for the ‘firm, written commitment’ (as detailed in my email below), to end of day this Friday, 29th October. After that time, I will open a new complaint.
I appreciate that the NHS is stretched due to rising Covid-19 cases, but we, service users, are seriously concerned by the discovery that while we were patiently waiting for the project to restart, believing that it had been postponed, both the CCG and AWP were actually carrying on with the work.
For speed of reference, I have attached a copy of the joint Terms of Reference for the ADHD Working Group.
Friday, 15 October 2021
Bristol Adult ADHD Support Group sent the following email to the CCG:
I have not yet received a reply to my email of Wednesday, 6 October (see below).
It has now been 10 months since our last meeting on 17 December 2020 and during these months, the CCG, unfortunately, has not been forthcoming with firm commitments for further meetings. The 5 February 2021 meeting was, understandably, postponed due to Covid-19 work pressures. But since then, despite promises of dates, nothing has happened other than that, as seen in current Board papers (some examples attached), the CCG and AWP have continued working on the Joint Collaborative ADHD Working Group project without the involvement of service users, contrary to the Working Group Terms of Reference.
I was sorry to hear that xxxxx is unwell, but I do not understand why our involvement in the ADHD project can only happen when there is a specialist handler present.
I remind you that AWP, the CCG, and xxxxx, xxxxx, and myself (as service user representatives) agreed to form the ADHD joint, multi-partner, collaborative working group in response to our formal NHS complaint filed on 6 December 2019. And it can clearly be seen from the Board Meeting extracts that our work is not finished.
Consequently, I have now been in contact with the Parliamentary and Health Services Ombudsman. I gave them a full and complete description and asked for their advice about how to proceed. They suggested I open a new formal NHS complaint.
I am seriously considering this. Since, however, I thought we were working well together up until February 2021, my preference would be for us to continue with the work without the distraction of a second complaint.
For this to happen, we need a firm, written commitment from the CCG and AWP. The written commitment must include firm meeting dates, a promise that postponements and cancellations will only happen after appropriate notice and after all three parties have agreed. In addition, the postponements/cancellations must have limited duration and limited frequency. Finally, the commitment must include a promise that we, the service user representatives, will receive copies of all relevant documents covering the work that was carried out by AWP and the CCG during the 10 months that we were not involved.
You should know that I gave the Ombudsman’s office permission to open a case file covering this situation in case it becomes necessary. I have the case number. I hope it won’t be needed.
Could you please reply by end of day on Monday, 25 October.
Thirty minutes later the CCG replied with an apology for the delay in replying to the Support Group’s email of 6 October and adding they are, ‘looking into this issue as a matter of urgency and will ensure we come back with a more detailed response as soon as possible.’
So fingers are now crossed!
Wednesday, 6 October 2021
Having not received any suggested dates from the CCG, the Support Group sent the following email:
Time is slipping by yet again! We have now been waiting about 9 months for a meeting date.
In another attempt to get things started, here are our dates:
They then listed several dates and asked the CCG to get back to them by end of day on Monday, 11 October.
Tuesday, 21 September 2021
The CCG replied to the Support Group’s email of 1 September saying they are,
currently looking at dates in October for a meeting to take place and will hopefully be able to get in touch next week with some suggested dates and times.
Wednesday, 1 September 2021
The CCG replied to the Support Group’s email of 27 August saying they needed to reschedule the next day’s meeting and asking for availability dates later in September.
The Support Group replied 20 minutes later giving the CCG their availability dates.
Friday, 27 August 2021
The Bristol Adult ADHD Support Group sent the following email to the CCG:
We still only have a holding invite for the proposed meeting date of 2 September for the ADHD Working Group. Could you please confirm that we will be meeting on this date?
I am asking this because I’m concerned to read in public documents that, contrary to our Terms of Reference, BNSSG and AWP have continued working together on ADHD matters after the working group sessions were put on hold. We, the service user representatives, were told the sessions were put on hold due to Covid-19 pressures.
In return, the Support Group received received bounce back holiday messages from key personnel at the CCG and AWP saying that they would be on annual leave during the first week of September, so the Support Group sent this follow-up email, on the same day, to the CCG:
I see from automatic replies (copies attached) that neither xxxx nor xxxxx would have been able to attend the proposed meeting date of 2 September. They are both on annual leave.
Could you please let me know what BNSSG intends for the proposed meeting on 2 September?
Also, if the meeting still goes ahead, will there be someone present from BNSSG who can provide us with written updates about the work done outside the working group?
Friday, 13 August 2021
The CCG replied saying that they had reviewed their colleagues’ diaries and suggested a meeting date of Thursday, 2nd September.
The Bristol Adult ADHD Support Group responded immediately and said they were available for the meeting on 2 September.
Wednesday, 11 August 2021
We heard nothing more from the CCG so today we sent the following email saying that we were pleased to see that the CCG agreed that it was ‘critical that we put in time as a group together to discuss how we move forward’ and gave them the dates for the remainder of this month and September when we are not available for meetings.
We added, as a gentle reminder, that ‘under the Terms of Reference (TOR) for our multi-partner, collaborative working group (agreed at the Local Resolution Meeting on 28 April 2020), the working group’s purpose and objective is not only to address the waiting list but also to devise an effective and sustainable ADHD service model; including a service user participation forum‘ and we attached a copy of the Terms of Reference.
We also attached copies of extracts from the CCG’s April 2021 Performance and Quality Report and the June 2021 Corporate Risk Register (both presented to the CCG’s Governing Body on 6 July 2021) to help illustrate that there is still work to be done to address the concerns raised in our original letter of formal complaint sent on 6 December 2019.
We finished by asking them to come back with some potential dates for meeting by end of day on Friday.
Shortly after, we received an email from the CCG saying they will check our dates against their calendar and ‘hopefully get something pencilled in.’ They apologised for the delay.
Fingers crossed!!
NB: It’s stated in the CCG’s Performance and Quality Report for April 2021 that the waiting list is now static at 3 years so we have accordingly amended the title of this post.
Tuesday, 13 July 2021
The CCG replied with a brief email thus:
Thanks for replying; as you say, it’s critical that we put in time as a group together to discuss how we move forward; once we have a clear picture of where the service is (current waiting list / demand, status of the LES in Primary Care etc), so that we can have something tangible as a group to work with. Will look into timelines and diaries and come back as soon as I can around this.
Monday, 12 July 2021
We replied to the CCG saying we were concerned with their statement that ‘AWP and CCG teams are currently working together to explore options for how we might address the long waiting lists’ because this is ‘being done without [service user] input which means not only is an important source of insight and information being overlooked, it is also contrary to our Terms of Reference. We can help with these actions and we want to help.‘
We also pointed out that while we appreciate that everybody has been working hard on Covid-19 related matters, our work on the ADHD waiting list and the ADHD service model has now been paused for 6 months.
Friday, 9 July 2021
We had heard nothing more from the CCG (since their last email of 3 May) until they sent us the following email on this date:
Further to [Bristol Adult ADHD Support Group’s emails of 6 & 21 April] and communications between us all in early June [NB: the support group was not a party to these June communications], I just wanted to provide a further update to you all. The working group sessions remain on hold; the ADHD service continues to see significant pressures with long waiting lists and resourcing issues, even when taking into account some additional funding offered by the CCG, this has made it difficult to make the tangible progress we would need in order to convene an effective working group session. AWP and CCG teams are currently working together to explore options for how we might address the long waiting lists which still exist for the service . . .Appreciate that it has been some time since we have all met as a group, but rest assured that this remains an absolute priority for both AWP and the CCG.
Monday, 3 May 2021
We received a follow-up email (to their email of 21 April) from the CCG saying they were ‘very keen to catch up with the full and core ADHD working group, but we do need to have progress made on the actions identified from our last meeting, otherwise we’re not making the most effective use of our collective time.
Whilst the immediate pressure of C19 cases is lower across the area, I believe there is still significant pressure on my colleagues from the commissioning team, as well as all of the AWP staff, so I suspect it will be another week or two before I’m able to get them to respond back to my requests.’
Wednesday, 21 April 2021
We resent our email of 6 April 2021 because we had not received a reply and on the same day the CCG replied that they were ‘linking in with colleagues to follow up on the actions we captured in our last working group session, to ensure we are able to make progress in our next meeting. Will be in touch with a further update as soon as possible.’
Tuesday, 6 April 2021
On this date we sent an email to the CCG asking if the ‘Covid-19 pressure has eased up enough that we can start considering dates for the next full working group as well as the core group meetings?‘ because we had not heard from the CCG about the promised March meeting.
Tuesday, 2 February 2021
We received an email from BNSSG CCG notifying us that they’d taken the decision to stand down the next scheduled meeting (Friday, 5 February 2021) and reschedule it for March because they were experiencing increased pressures on local NHS and care system, as coronavirus cases continued to rise and more people required hospital treatment.
Up until this date, we had been working diligently towards resolving the waiting list issue and reviewing the service model. We will be continuing this work when Covid-19 pressures allow.
Tuesday, 28 July 2020: Good News
The Bristol Adult ADHD Support Group, the Bristol, North Somerset & South Gloucestershire CCG (BNSSGCCG) and Avon and Wiltshire Mental Health Partnership NHS Trust (AWP) have been working together, at pace, in a joint, multi-partner, collaborative working group with the dual purpose of addressing the waiting list issues as a priority while, at the same time, methodically analysing problems that led to the waiting list and then devising and implementing solutions.
The end goal of the working group is to have an Adult ADHD Service that assesses people within the 18 week target and is cost effective (now and in the future), that effectively and efficiently integrates care, is high quality, safe and gives service users a positive experience. It will meet legal duties, NHS Quality Board’s definition of quality (safe, effective, caring, responsive and person-centred), as well as NICE Guidelines & Standards.
It will be an Adult ADHD Service that everyone can be proud of!
On Friday, 5 June 2020, formal Terms of Reference for the working group were adopted and we agreed ways of working and communicating.
The Core Working Group (CWG) is now having weekly working meetings and is updating the Full Working Group (FWG) on a monthly basis. In turn the FWG is giving monthly progress reports to the CCG’s Commissioning Executive Committee (CEC) for their feedback and/or approval. BTW: we are all working & meeting online & we are working well together.
We are working as hard and fast as we can while balancing accuracy with speed. The waiting list is an urgent priority.
We will periodically update this page with progress reports.
Monday, 17 February 2020
I’m afraid we were overly optimistic as progress seems to have stopped so today I sent two emails as follows:
First email:
I realise that everyone is busy but it has now been 3 weeks since I sent the list of dates for which we are unavailable for a meeting and I have not yet had a reply.
Do you know if any progress has been made in arranging this meeting with the CCG, [Clinic staff], members of the joint CCG and AWP ADHD Working/Project Group, and [seAp Advocacy]?
To date, it is 6 years and 10 months since the funding level for the clinic was set and it has been 5 years and 10 months since the then Bristol CCG recognised that the funding level was inadequate.
Furthermore, the Bristol Adult ADHD Support Group met on Friday, 14 February, and it rapidly became apparent that the waiting list (2 years and growing), without any doubt, is putting already distressed people at increased risk of harm. In addition, the group members already assessed strongly reiterated their support for the clinic as well as their high regard for the staff whilst also expressing concern that the ever increasing waiting list is now putting too much pressure on the service as a whole.
As a polite reminder, I have reattached my original letter of Friday, 6 December 2019; sent 2 ½ months ago. Everything stated in this letter regarding the CCG’s responsibilities as well as our offer of help still stands.
Please note, I have also cc’d Mr John Penrose, MP on this email since I understand he is making enquiries into the inadequate funding for NHS ADHD services on behalf of constituents and I am also his constituent.
Second email:
43 working days have now passed since you received my FOI Request.
During that time the deadline for the CCG’s response has been extended twice from the original date of Tuesday, 14 January 2020; first to Tuesday, 28 January (need time to finalise the response) and then again to Monday, 3 February 2020 (for review by a Director).
It has now been 10 working days since the CCG’s last deadline expired. Could you please, therefore, conduct an internal review into the handling of this matter. My original request for information can be read at the end of this email chain.
Wednesday, 22 January 2020
We’re making progress, slow inching progress, but progress nevertheless. We filed a Freedom of Information request with BNSSG CCG on 12 December 2019 for documents they described in their minutes (discussions about the Adult ADHD service) but had not made available online. The CCG, in response, told us they needed more time to ‘finalise’ their response and they expected to release the information by 28th January.
As a result, we’ve asked that our meeting take place in mid February so that we have time to review the documents. And we’ve listed the other people that the CCG needs to invite to the meeting ‘in the interests of transparency and because [the waiting list] is a very serious problem that needs an open and collaborative partnership between the CCG, AWP, and service users.’
Thursday, 9 January 2020
Since we filed our complaint with Bristol, North Somerset and South Gloucestershire Clinical Commissioning Group (BNSSGCCG) on 6th December 2019, some progress has been made as follows:
1.BNSSGCCG have proposed that they hold a meeting this month (date tbd) with us (service users), the ADHD Clinic staff, and others from Avon and Wiltshire Mental Health Partnership NHS Trust (AWP). We are now waiting to hear from all attendees.
2. The CCG have also sent a proposed agenda which needs some amendments.
3. We have notified Healthwatch Bristol, North Somerset and South Gloucestershire (Healthwatch BNSSG) about the problems with the waiting list and sent them a copy of our complaint. We will be talking with them tomorrow, and they will be investigating the issues around the waiting list. We have also been in communication with Healthwatch England who are aware of our complaint. Healthwatch England have said that they will assess and evaluate the results of Healthwatch BNSSG’s investigation for national implications.
Saturday, 7 December 2019
The waiting list for the Bristol NHS Adult ADHD Clinic is now 2 years (plus) for people living in Bristol. We weren’t sure what Bristol, North Somerset and South Gloucester Clinical Commissioning Group (BNSSGCCG) were doing about it, if anything, so we decided to try and find out.
First, here’s a little bit of background. Clinical Commissioning Groups (CCGs) were created in 2012 when the new Health and Social Care Act came into being and they opened their doors on 1 April 2013. The CCGs are membership bodies made up of the local GP practices and they are led by a governing body also made up of GPs some clinicians, nurses and lay people. The CCG buys (commissions) all the health services (physical & mental health) that we use within our local areas. For example, the BNSSGCCG has a contract with Avon & Wiltshire Mental Health Partnership NHS Trust (AWP) for the Adult ADHD service for all who it in the Bristol, North Somerset and South Gloucestershire Area.
Now before buying a service such as the ADHD Clinic, the CCG should determine the level of need in the community as well as the amount of funding they’re going to need for the service currently and into the future. In other words they need to plan for increasing demand They should also plan for future demand as people become more aware of ADHD and ADHD services. And this is where things can go wrong as it has done for BNSSGCCG.
In 2013, for whatever reason they didn’t plan for the number of people in the greater Bristol area who would need an ADHD service and they didn’t pay attention to the increasing number of people being referred to the clinic and they didn’t listen to the Clinic’s warnings. And now there’s a very long waiting list.
And now we go back to where we left off in the first paragraph of this post: we were going to do some research. We did, and didn’t like what we found, so yesterday we sent BNSSG a letter with an appendix containing 33 pages of evidence. The appendix can be read here and the letter is below:
6 December 2019
Dr Jonathan Hayes, Clinical Chair
NHS BNSSG Clinical Commissioning Group
South Plaza
Marlborough Street
Bristol
BS1 3NX
Dear Dr Hayes,
Re: OPEN LETTER: Serious concerns about BNSSG’s handling of the Adult ADHD Service waiting list
I am the Chair of AADD–UK and the founder and facilitator of Bristol Adult ADHD Support Group; both running continuously for 12 years. I’ve contributed to the NICE ADHD Guidelines and Quality Standards and I’m a member of the NICE ADHD Implementation Group. The latter was charged by the Department of Health and Social Care with highlighting challenges and developing solutions for implementing NICE NG87 ADHD. Commissioners are responsible for enabling patient use of the Guidelines not only within the context of funding but also within context of their legal duties of eliminating discrimination, advancing opportunities and reducing health inequalities.
I am writing this letter on behalf of service users who potentially have ADHD as well as those who have the diagnosis. The Bristol Adult ADHD Service does not know that I am writing this but as a matter of courtesy I have sent them a copy. The number of people expressing distress about the length of the waiting list for the Bristol Adult ADHD Service is steadily increasing. Since I needed to understand the background to this situation, I read all available BNSSGCCG’s minutes and reports. And I now have very serious concerns about BNSSG’s management of the waiting list.
In April 2014, one of the CCG’s operational delivery projects for the ADHD service was to ‘achieve funding’ to resource its then current growth. Since that date, referrals have risen exponentially but the CCG left the funding at the 2013 level—despite receiving warnings from the service. They have also been underspending on ADHD services to help offset overspending on IAPT and mental health placement commitments. The Clinic staff from 2014 to date, continuously tried to increase capacity to match the ever-growing demand until it seems they could do no more. The CCG refused to increase funding and favourably compared the 2-year ADHD wait time (keeping ‘inappropriate costs’ down) with the 2-week wait time for Cataract surgery. Furthermore, there’s no evidence the CCG made any effort to understand the needs of people with ADHD. There’s also no evidence of engagement or involvement with patients. See Appendix A for details, comments (blue text), as well as questions for the CCG (green text) to answer.
The CCG’s decisions and actions means it is violating the principles, values and objectives as set out in their ‘Constitution’, their ‘Equality, Diversity and Inclusion Strategy’, their ‘Ethical Framework for Decision Making’, their ‘Procurement Policy’ as well as the ‘NHS Constitution’, the statutory guidance for ‘Patient and Public Participation in Commissioning Health and Care’ and the ‘Good Governance Standard for Public Service’.
Furthermore, these decisions and actions have potentially put the CCG at risk of being in breach of their legal duties to reduce inequalities, eliminate discrimination, promote involvement of patients and obtain appropriate advice as set out in the Health and Social Care Act 2012 and the Equality Act 2010.
First, I ask the CCG to review their decisions and actions in line with these principles, values and legal duties and to make amends. Secondly, I ask the CCG to answer my questions in Appendix A.
I have written this letter, however, not just to express my serious concerns and to ask for amends, but also to offer my help to the CCG. I can help the CCG understand the importance of a fully functioning Bristol Adult ADHD Service. Indeed, it is held in high regard by service users. Appendix C contains lists of service user comments extracted from the ADHD Service’s quarterly and annual reports (released by the CCG in response to a Freedom of Information request). I can confirm the compliments in these lists match the feedback I hear at support group meetings as well as those from my networks. If anyone at the CCG is interested in learning about the lived experience of ADHD, I can help with that too. In fact, I am willing to invite relevant personnel to support group meetings so that they can directly hear from others about their needs.
ADHD is a serious neurodevelopmental disorder that can affect about 2-4% of adults. It is complex and difficult to diagnose. Many adults who were not diagnosed in childhood or were misdiagnosed will have developed co-existing disorders which act to amplify the symptoms and increase the complexity of assessments and diagnosis. ADHD symptoms can cause significant impairment across all domains of adult life (e.g. interpersonal relationships, education and work) and negatively impact health-related quality of life. It is cost effective to fund appropriate and timely treatment.
Please respond by Friday, 20 December 2019. I am currently considering further actions.
Yours sincerely,
Appendix A: Timeline – Serious Concerns about BNSSG’s handling of the Adult ADHD Waiting List
ADHD, BPS & Power Threat Meaning Framework
YET ANOTHER UPDATE TO OUR, SO FAR, FRUITLESS COMPLAINTS TO THE BPS:
Thursday, 12 December 2019:
We sent the following email to BPS:
Did the Trustees ever finish investigating my complaint about the way ADHD is stigmatised in the Power Threat Meaning Framework.
To date, the PTMFramework is still available on the BPS website and still contains demeaning statements about people with ADHD.
I realise 11 months have passed so for speed of reference, I’ve reattached my original documents as well as additional documents showing that BPS has actively promoted the framework.
Tuesday, 9 July 2019:
As of today, we’ve heard nothing from anyone at The British Psychological Society (BPS) regarding their investigation of our complaint about the stigmatisation of people with ADHD in The Power Threat Meaning Framework (PTMF). You can read the history of this sorry matter under ‘Past Events’ at the end of this post as well as in the ‘Featured Posts’ below this one.
We are now preparing to escalate our complaint.
To be frank, we feel surprised, and yes a bit hurt, that we haven’t heard from BPS because it really wouldn’t have taken much effort on their part to discover that the authors of the PTMF are in fact ADHD deniers.
See for example this 2016 tweet from the lead author:
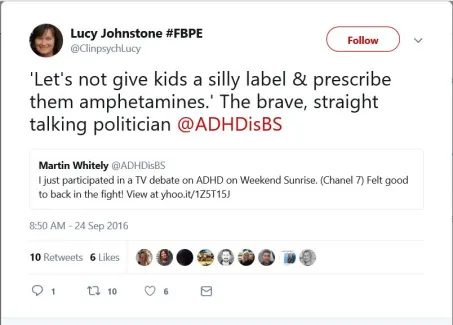
and this 2018 tweet from another PTMF author:
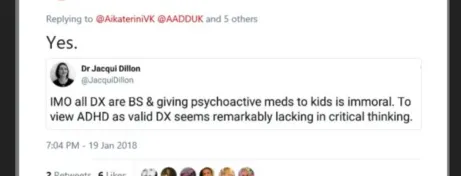
There are plenty more examples from others, but you get the picture.
The authors, of course, as private individuals have the right to their opinions and have the right to publish them under their own names. But the PTMF, as it states on the copyright page, was printed and published by The British Psychological Society, BPS owns the copyright and their logo tops the cover page.
In the document summary on page 5, the authors have explained how the PTMF came about thus:
In 2013, the Division of Clinical Psychology (DCP) of the British Psychological Society (BPS) published a Position Statement entitled Classification of behaviour and experience in relation to functional psychiatric diagnoses: Time for a paradigm shift. Recommendation 3 of the position paper is: ‘To support work, in conjunction with service users, on developing a multi-factorial and contextual approach, which incorporates social, psychological and biological factors’ (p.9). This document is the result of a DCP-funded project for work towards fulfilling this aim.
And here is the British Psychological Society promoting the one year anniversary of the launch of the PTMF:

Seems pretty clear that the PTMF has been published under the aegis of The British Psychological Society thus endorsing and legitimising the authors’ lack of knowledge about neurodevelopmental disorders as well as their disrespectful & discriminatory attitude towards people with ADHD.
It shouldn’t be necessary for us to draw the attention of the BPS and the authors to the ethical principles in BPS’ Code of Ethics but since it is, here are two quotes from page 5 they may want to start with:
Respect for the dignity of persons and peoples is one of the most fundamental and universal ethical principles across geographical and cultural boundaries, and across professional disciplines.
Statement of values: Psychologists value the dignity and worth of all persons, with sensitivity to the dynamics of perceived authority or influence over persons and peoples and with particular regard to people’s rights.
They might also want to reflect upon this quote from page 2:
Ethical reasoning is often subject to various competing biases. Maintaining awareness of such biases is important when trying to think through ethical challenges. These considerations currently include but are not limited to, salience (how readily something comes to mind), confirmation bias (the human tendency to look for evidence that confirms their belief and to ignore other evidence), loss aversion (behaviour to avoid loss), beliefs about disclosure (tendency to be more honest when they believe their actions will be known by others), and dissonance reduction (acting to maintain consistent beliefs). This list will evolve over time with the advancement of knowledge in this area. Psychologists are therefore well placed and encouraged to consider these factors in their own decision-making.
We would also urge BPS and the authors to begin thinking about this quote from page 3:
Psychologists should consider it good practice to record their decision processes when confronted with a particularly challenging ethical issue so that it is available for future reference if that decision is re-visited.
As I wrote at the beginning, we’re preparing to escalate our complaint!
PS: Here’s a link to The British Psychological Society’s Code of Ethics and Conduct.
PAST EVENTS
On Monday, 14th January 2019, we received an email from the Governance Manager of the British Psychological Society letting us know that a Director of the Society has been appointed to investigate the issues we have raised and that the investigation will take 4 weeks to complete.
On Wednesday, 2nd January 2019, we received the following reply from the Governance Manager at BPS:
Your complaint as set out below has been forwarded to me for attention. I am very sorry to learn of your concerns
I am making enquiries into the matters which you raise and I will be in touch as soon as my enquiries are complete
Kindest regards
On Sunday, 9th December 2018, we sent the following email to the Chief Executive and Trustees of the British Psychological Society (BPS):
Dear Mr Bajwa and Trustees of the British Psychological Society,
I would like to bring to your attention the harmful manner in which Attention Deficit Hyperactivity Disorder is referenced in the document titled ‘Power Threat Meaning Framework’ (PTMFramework).
Lucy Johnstone, lead author, on 30 November 2018 told us on Twitter that all discussions of ADHD had been specifically excluded from the PTM Framework (see attached: ‘Tweets September to 30 November 2018’). But to date, the uncorrected version of the PTM Framework ( i.e. the version containing 16 references to ADHD, all of which are stigmatising and harmful) is still on the British Psychological Society’s website here https://www.bps.org.uk/news-and-policy/introducing-power-threat-meaning-framework
If you are able, please could you provide us with a copy of the amended version of the Framework and ensure that the uncorrected copy is replaced?
If it has not been amended, please could you discuss this matter with the Trustees as to whether or not the Framework meets the requirements of the BPS Royal Charter.
Sadly, we have some doubts as to whether the Framework has been amended as Lucy Johnstone and her fellow authors are adamantly opposed to psychiatric diagnoses as illustrated in one of the attached tweets as well as in the following quote from the 3rd paragraph on page 314 of the PTM Framework:
At the same time as affirming people’s right to describe their difficulties as they wish, we affirm the equally important principle that professionals, researchers, trainers, lecturers, charities, policy-makers and others involved in the mental health field should use language and concepts that have some claim to be descriptively accurate and evidence-based. Because psychiatric diagnosis does not meet these standards, it follows that it can no longer be considered professionally, scientifically or ethically justifiable to present psychiatric diagnoses as if they were valid statements about people and their difficulties. To draw an analogy from psychiatric history, once it becomes clear that terms like ‘wandering womb’ are mistaken, no professional should be offering – let alone imposing – them.
For your information here is some background:
In January 2018, the launch of the Power Threat Meaning Framework was heavily promoted on Twitter under #PTMFramework and as part of the launch it was also advertised as being available on the British Psychological Society’s website. As a result of this we, Adult Attention Deficit Disorder-UK (AADD-UK), became aware of the published document so we downloaded the full version (414 pages) and read it.
There are 16 specific references to Attention Deficit Hyperactivity Disorder (ADHD) in the framework (see attached document) which are in themselves incorrect and when read in the context of the framework as seen in the quote above.
We’ve given our feedback to the authors many times since the launch of the PTM Framework, but until 30th November 2018 it has been consistently ignored. Please note that while Lucy Johnstone says she won’t engage in a debate about the framework, she is still actively promoting it on Twitter.
We are bringing this to your attention as well as the attention of the trustees not only because Lucy Johnstone directed us to the BPS but also because the presence of the BPS Logo on the Framework lends credence and validity to statements which stigmatise people with ADHD.
If you have any questions, please do not hesitate to contact me. I’m very willing to help.
Here is a link to the copy of some tweets we sent to the BPS, Tweets September to 30 November 2018
Here is a link to a list of the statements in the Power Threat Meaning Framework that we sent to the BPS, Quotes from PTMF for Letter
And finally, if anyone is interested in reading more, here is a link to the 414 page version of the Power Threat Meaning Framework: Towards the identification of patterns in emotional distress, unusual experiences and troubled or troubling behaviour, as an alternative to functional psychiatric diagnosis
Shine a light – understanding ADHD
“I feel like a universe, stuffed within a shoebox” – this is how Bryn Travers describes what it’s like to have Attention Deficit / Hyperactivity Disorder (ADHD). On 31st October 2018 the video ‘Shine a light – understanding ADHD’ was released: it’s a short documentary about what ADHD is, both from a personal and from a clinical perspective.
The release of this video co-occurred with the last day of the international ADHD awareness month (October). This initiative of the international ADHD patient organisations aims to raise awareness about ADHD, as well as funding for more research to better understand ADHD. Many events were organised worldwide during October to inform people about ADHD. Knowing more about ADHD and spreading awareness will help people to better understand (people with) ADHD. This will reduce stigma and (self)blame.
The video is in English, with subtitles in English, German, Dutch, Italian, Spanish, Hungarian and Swedish.
What is this video about?
Many children, adolescents and adults suffer from ADHD. ADHD is a complex disorder that affects people differently. Generally people experience problems in daily life, especially with respect to controlling attention, impulses and emotions. At the same time, people with ADHD enjoy their creativity and positive energy. Medication is effective for many people with ADHD, but not for all. A downside of the medication is that it needs to be taken every day, and it does not cure someone from the disorder. Other types of treatment should therefore also be offered and investigated. Knowing more about ADHD and spreading awareness will help people to understand what causes their behaviour. This will reduce stigma and (self)blame.
The makers of this mini-documentary have asked people with ADHD and their relatives what is like to have ADHD, what are the challenges and what are the things they like about ADHD. They have also asked clinicians and researchers working with ADHD to explain more about the origins of the disorder, what they have learnt from their experience working with patients, but also what are the main questions that research is trying to answer about ADHD.
Who is in the video?
The video features four of the most well-known researchers in the field of ADHD:
Dr. Eric Taylor is Emeritus Professor of Child and Adolescent Psychiatry at King’s College London,
Dr. Philip Asherson is professor of Molecular Psychiatry at King’s College London,
Dr. Barbara Franke is professor of Molecular Psychiatry at Radboud University Medical Center Nijmegen, in The Netherlands, and
Dr. Corina Greven is psychologist and behavioural geneticist at Radboud University Medical Center Nijmegen.
Next to these scientists and psychiatrists, we see three people with ADHD:
Bryn Travers, Evie Travers, and Aziz.
And we also see:
Andrea Bilbow, President of ‘ADHD Europe’ and mother of two children with ADHD,
Dr. Kai Syng Tan, researcher and artist at King’s College London, who also has an ADHD diagnosis.
In the video they talk about what ADHD is and what it is like to have ADHD, about the pro’s and con’s of ADHD medication and why other types of treatment should also be developed, about stigma and misconceptions and why education is so important, and about the positive aspects of ADHD.
About the collaborators of this video
This video was a created through collaboration between four EU-funded, international consortia of researchers that investigate ADHD and its origins. The idea came from two junior scientists, Laura Ghirardi and Dr. Nicoletta Adamo. They were supported in creating the video through the MiND Training program and by the other junior scientists from MiND.
More information about the researchers and consortia:
Aggressotype (origins of aggression in psychiatric disorders, such as ADHD):
CoCA (origins of comorbid disorders with ADHD in adolescents and adults):
Eat2BeNICE (how nutrition and lifestyle influence mental health in psychiatric disorders)
The video was recorded by 4QUARTER FILMS
ADHD Celebration Day in Bristol
Celebrating the achievements and diversity of adults with Attention Deficit Hyperactive Disorder (ADHD):
 Avon and Wiltshire Mental Health Partnership NHS Trust (AWP) is inviting adults with ADHD, in Bristol & greater area, to an awareness raising and recognition event.
Avon and Wiltshire Mental Health Partnership NHS Trust (AWP) is inviting adults with ADHD, in Bristol & greater area, to an awareness raising and recognition event.
The Trust’s Adult ADHD Service is aiming to celebrate neurodiversity, help build resilience and galvanise a wider ADHD community through its event on Friday 12 October, which will showcase the successes and skills of adults with the condition.
Dietmar Hank, Consultant Psychiatrist in Adult ADHD for AWP, said: “People with ADHD can live very successful and fulfilled lives. A thorough assessment, education/knowledge about the condition and appropriate treatment are often the key to positive changes. ADHD doesn’t just affect those with a diagnosis. Families, loved ones, friends and wider society can struggle to make sense of the condition and some of the problems caused by it.
“We want to focus on the diversity and strengths many people with ADHD demonstrate and give adults with the condition the opportunity to meet others, learn from and share with each other.”
The event, which is taking place at the Trinity Centre, Trinity Road, Bristol, BS2 0NW, from 10am until 3.30pm, will feature workshops, talks delivered by people affected by ADHD, music and much more. It is open to adults with ADHD (in Bristol & greater area), their friends and family, professionals and other interested parties.
More details are here on Avon and Wiltshire Mental Health Partnership NHS Trust (AWP)’s website.
British Psychological Society endorses stigmatisation of ADHD
D: Second Update to Original Post (see A, B & C below)
Thursday, 7th June, We’ve just learnt that it looks as if the Power Threat Meaning Framework has been adopted as policy by the Division of Clinical Psychologists at the British Psychological Society. An email has been received by other psychologists which says “Statements of Interest are invited to join the DCP Power Threat Meaning Framework (PTM) Working Group, that reports directly to the DCP Committee.”
We have been working hard on our report about the PTMFramework and are now compiling the results into a coherent whole so that it can be presented along with our letter of complaint. This has not been easy and has taken a while as the Framework itself is a poorly researched and poorly written mishmash of outdated ideas as well as being unintelligible in sections.
C: Second Update to Original Post (see A & B below)
As of today, Monday, 30th April, we’ve still not had any kind of a reply from the British Psychological Society regarding their stigmatising and discriminatory attitude towards people with ADHD. We sent the BPS & authors of the Power Threat Meaning Framework a note today, via Twitter, to say that unless they promise by Friday, 4th May, in writing, that ADHD will be deleted from the PTMFramework we will be taking further action.
FYI, work on this further action is well underway!
In the meantime, we note that Lucy Johnstone, a consultant clinical psychologist and one of the two lead authors of the framework, tweeted at 5:10 pm on Tuesday, 24th April the following:
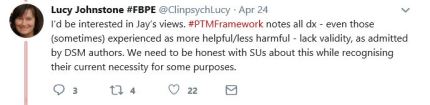
As you see, Lucy Johnstone declares that all diagnoses lack validity even if people actually find them to be helpful. And she says, psychologists should be honest and tell us that our diagnoses are invalid. That is an arrogant and harmful statement that devalues the experience of service users.
And before any of the authors think about contacting us to claim that the PTMframework is an alternative option to the DSM (Diagnostic and Statistical Manual of Mental Disorders), we will state right here and now that we are not fooled! At the same time they tell everyone that their framework is an alternative option, they also deny the validity of the DSM. No options allowed!
Basically, in the PTMframework the authors claim that the symptoms we experience (ADHD included) are expressions of emotional distress caused by “relational and social adversities” such as poverty, discrimination, inequality, violence and abuse. Furthermore, they state that there are no ” consistent associations between functional psychiatric diagnoses [e.g. ADHD] and any biological pathology or impairment, and nor have any biomarkers been identified” (Johnstone, 2018, 7). In short, the authors dismiss the results of genetic and screening research. The framework is not backed by reliable research and the authors lack the depth of knowledge and experience of the DSM authors.
While the framework may be helpful for those people whose distress has been solely caused by relational and societal adversities (although they will still need the utility of the DSM), it will not help those whose distress results from the impact of complex interactions between genetic and environmental influences amplified by relational and societal adversities. In fact, in these instances the framework will only serve to disempower people by denying the validity of their experiences. It will increase feelings of failure and despair.
Unlike the PTMFramework, the DSM is designed as a classification system that provides cross-border mental health professionals with a common diagnostic language that is useful for both treatment and research efforts. While some of the DSM authors recognise that it is a flawed system, in part because knowledge about mental ill health is evolving and changing, they also acknowledge that the DSM contains much practical information and experience and is better than anything else currently available (and when used properly does a good job).
The two main criticisms levelled against the DSM (and psychiatry in general) are first, that it medicalises normal behaviours and turns them into illnesses and disorders to be treated with drugs and secondly, that the DSM’s authors (and psychiatrists in general) have conflicts of interest because they have links with the pharmaceutical industry.
The critics, including the authors, using these arguments conveniently overlook the fact that researchers from both the medical field and the pharmaceutical industry need to work together in order to find and develop effective treatments. They overlook the fact that in the UK the pharmaceutical industry is heavily regulated. Additionally, as we’ve noticed with the BPS and some of their members, many of these same critics fail to declare their own financial and personal interests.
Please don’t misunderstand us. We’re not against debating the meaning and definition of illness and disorder, we’re not against improving the validity of specific diagnoses, we’re not even against changes to the classification system; so long as changes are in line with improvements in knowledge about causes of and experiences with mental ill health.
We are, however, against mental health professionals working outside their area of expertise and not declaring their lack of knowledge. We are also against the same professionals resorting to misinterpreting the conclusions of more knowledgeable colleagues and making attention-grabbing and unfounded pronouncements such as the ones they make about psychiatrists and psychiatric diagnoses. The authors allege that psychiatric diagnoses are neither descriptively accurate nor evidence-based and cannot be considered “professionally, scientifically or ethically justifiable” (Johnstone, 2018, p. 314). We are against mental health professionals attempting to enhance their own professional reputation by using these sorts of tactics to discredit the work of other colleagues.
Additionally, we think it is unethical and unprofessional, to say nothing of being harmful, for the authors of the PTMFramework to justify their own work by perpetuating distrust of psychiatry amongst people with negative experiences and by undermining the trust of those who’ve had helpful experiences.
Finally, we will point out to all those mental health professionals who feel disturbed by the implications of the PTMFramework but are staying silent, thereby implying acceptance, the framework authors’ failure to recognise their own limits, biases, prejudices, professional and power interests will not only cause harm to many service users, it will also damage the reputation of psychology as a helpful profession. And those of you who do not speak up will be seen as complicit.
There will be more on these as well as additional points later!
B: First Update to Original Post (see A: below):
As of today, Tuesday, 27th March 2018 we’ve had no reply whatsoever from the British Psychological Society. Never mind; we’ve been working hard on a comprehensive follow-up which we will send to certain parties as well as publish here.
In the meantime, we note that on 1st March 2018 Lyn Romeo, Chief Social Worker for Adults, at the Department of Health not only introduced the Power Threat Meaning Framework as a “radically different perspective on mental health“ on her official government blog but also allowed Phil Wilshire, principal social worker for Avon and Wiltshire NHS Partnership Trust to write a guest blog promoting the framework.
Phil does acknowledge that some professionals and some service users have been critical of the framework so he tries to argue that the framework is an “optional conceptual resource” and that it is not anti-medication. His efforts, however, are deliberately misleading given that in the first paragraph on page 314 of the framework the authors clearly state that while they affirm “people’s right to describe their difficulties as they wish, we affirm the equally important principle that professionals, researchers, trainers, lecturers, charities, policy-makers and others involved in the mental health field should use language and concepts that have some claim to be descriptively accurate and evidence-based. Because psychiatric diagnosis does not meet these standards, it follows that it can no longer be considered professionally, scientifically or ethically justifiable to present psychiatric diagnoses as if they were valid statements about people and their difficulties.” You see; they are actually trying to take away our right to accept our ADHD diagnoses by calling them unprofessional, unscientific and unethical. What’s more they haven’t provided any valid evidence at all for this opinion.
By the way; Phil Wilshire probably should have declared his interest in the Framework as he’s listed on page 3 as having “significant input into Chapter 8” which is titled “Ways forward” and contains the following sections: 1. Public health policy. 2. Mental health policy. 3. Service principles. 4. Service design, commissioning and outcomes. 5. Access to social care, housing and welfare benefits. 6. Therapeutic interventions. 7. The legal system. 8. Research. 9. Use of language.
Mr Wilshire, of course, is advocating an eventual “collective shift towards a non-diagnostic paradigm.” (p. 264) Well . . . . good luck!!
And just in case Phil and Lyn have been chatting about how to implement the Framework, we suggest that since they both work for public bodies, they might like to ask themselves how their support for the framework complies with their public sector equality duty under the Equality Act 2010. And if they’ve overlooked their legal obligations, here’s a reminder: “those subject to the equality duty must, in the exercise of their functions, have due regard to the need to: Eliminate unlawful discrimination, harassment and victimisation and other conduct prohibited by the Act. . . etc.“!!!
A: Original Post (rev. edn. published 26th January 2018):
On Tuesday, 16th January, AADD-UK was alerted to a furious Twitter row that began Friday, 12th January when the Division of Clinical Psychology (DCP), a Division within the British Psychological Society (BPS),* held an actively promoted launch at the Friends House, across from Euston Station, London for the Division’s recently published “Power Threat Meaning Framework: Towards the identification of patterns in emotional distress, unusual experiences and troubled or troubling behaviour, as an alternative to functional psychiatric diagnosis.”
Having no idea what this Framework was about & curious as to why there was such a ruckus, I downloaded a copy and began reading.
This is what happened:
The Framework seemed sturdy, 411 pages long, and reputable. It’s on the BPS website, it has their logo (Tagline: Promoting excellence in psychology) as well as the logo for the Division of Clinical Psychologists. It’s clearly stated on the printer’s imprint and copyright page that the publication “has been produced by the British Psychological Society’s Division of Clinical Psychology as a Member Network publication and represents the views and expert contributions of its authors” and it was printed and published by the British Psychological Society.
So far so good.
Next, on page 5, under the heading ‘Document summary‘, I learnt the reason for the existence of the Framework as follows (please bear with me as I give you these somewhat tedious details, their relevance will be more evident later):
In 2013, the Division of Clinical Psychology (DCP) of the British Psychological Society
(BPS) published a Position Statement entitled “Classification of behaviour and experience in relation to functional psychiatric diagnoses: Time for a paradigm shift.” Recommendation 3 of the position paper is: ‘To support work, in conjunction with service users, on developing a multi-factorial and contextual approach, which incorporates social, psychological and biological factors’ (p.9). This document is the result of a DCP-funded project for work towards fulfilling this aim.
Since I tend to be overly conscientious as well as curious, I decided to read ‘Time for a paradigm shift‘ first so that I could understand the context for the PTMFramework so I downloaded a copy, thankfully only 9 pages long, and began reading (it’s publication format was the same as the Framework’s).
I was more interested when I recognised a few of the author’s names due to their interactions with the Twitter row. Things quickly became more interesting when, on page 2, I read the following paragraph (emphasis mine):
At the same time it should be noted that functional psychiatric diagnoses such as schizophrenia, bipolar disorder, personality disorder, attention deficit hyperactivity disorder, conduct disorders and so on, due to their limited reliability and questionable validity, provide a flawed basis for evidence-based practice, research, intervention guidelines and the various administrative and nonclinical uses of diagnosis.
After this, I carried on reading, paying closer attention to the references and source names, some of whom I also recognised, and by the time I reached the summary (below) on page 5, I’d already concluded that the ‘position statement‘ produced by the Division of Clinical Psychologists was a veiled attempt at undermining psychiatry and diagnoses, i.e. anti-psychiatry. The Twitter row wasn’t the only place I’d seen those names.
The DCP believes there is a clear rationale and need for a paradigm shift in relation to functional psychiatric diagnoses. It argues for an approach that is multi-factorial, contextualises distress and behaviour, and acknowledges the complexity of the interactions involved in all human experience.
The whole Division? I wondered how many psychologists were involved so I did a Google search. I didn’t find numbers for psychologists but I did find an interesting page on the BPS website under “news”. It’s titled “The future of clinical psychology in the Society” which mentions plans for a another UK association for Clinical Psychologists. Intriguingly, there’s strange hints about unity (lack of?) along with a reminder that relationships with external organisations must advance BPS’ objects. The policy is linked to this page. Hmm! Keep all this in mind as you read on.
I returned to reading the Power Threat Meaning Framework. Now, I freely admit that I was slightly distracted by the policy I’d just read and I was aware my bias filters were turned on. I thought I knew what to expect. I was wrong!
I was shocked! And this feeling intensified the more I read. The authors’ tone, conveyed through their choice of words and viewpoint, is arrogant and patronising and their negative and disapproving attitude towards ADHD is stigmatising and discriminatory. Make no mistake the ideology behind the Framework belongs to the anti-psychiatry movement.
I’m not going to analyse the arguments put forward in the Framework other than to say that while some of the ideas are interesting, they aren’t discussed in any depth. The authors’ make some half-hearted attempts at describing different sides of an argument, but these are often spoilt by their habit of using adverbs to manipulate us into choosing their favoured option .
This post is getting too long so I’m only going to add 5 extracts from the Framework so that you have some sort of idea as to what it’s like. I’ve put links to the Framework as well as to the Time for a Paradigm Shift at the very end of this post in the References section. If you’re interested, you can download them and judge them for yourselves.
“. . .and psychiatric diagnoses are often explicitly used as explanations. But the impression of explanation is false and the reasoning behind it is illogical“. (2018, p.29)
“We underestimate the difficulty of describing patterns in people’s behavioural or bodily problems and often ‘see’ associations which are not there (known as the illusory correlation). This is why medical researchers have developed the kind of rules we discussed earlier to try to ensure that the bodily patterns they describe are ‘real’ and not illusory. The combination of limited public understanding of diagnostic procedures and overconfidence in judgements of patterns, can confer credibility on psychiatric categories which is not justified by the evidence“. 2018, p.30)
“The existence of particular categories can influence how people’s experiences are interpreted and how they express their distress. Aided by the illusory correlation, diagnostic categories can then become self-fulfilling prophecies, conferring further credibility as growing numbers of people seem to match them. And, especially if people do not have access to non-medical, non-blaming explanations, the process can become self-perpetuating as people increasingly request confirmation of self-diagnoses of ‘bipolar disorder’ or ‘ADHD’ and so on.” (2018, p.30)
“All of this is reflected in psychiatric diagnosis’ inevitable dependence on social judgements, as we discussed in Chapter 1, and many critics have traced particular diagnoses back to the social norms they challenge: ‘borderline personality disorder’ for women who are too angry; ‘depression’ for women who are exhausted by domestic demands; ‘anorexia nervosa’ as a reaction to the unrealistic role and appearance standards faced by modern women; alcohol misuse and suicide for men whose socialisation does not permit the expression of despair in other ways; ‘ADHD’ for children who are not suited to educational regimentation, and so on . . .These rule transgressions can involve over-adaption to the ideal image, as well as failing to live up to it; . . . Similarly, it has been suggested that the enormous rise in diagnoses of ‘autism spectrum disorders’ and ‘Asperger’s’ may partly reflect demands made by highly industrialised and service-oriented economies for successful employees to display emotional behaviours such as (faked) sociability, warmth, gratitude, passion and so on – skills which do not come easily to everyone (Roberts, 2015). (NB: Although autism in its most severe forms fits the profile of a neurodevelopmental disorder of some kind, the debates about these diagnoses are particularly complex . . . Given all this, it is hardly surprising that in many parts of the Global South, there may be no equivalent categories to the experiences that DSM and ICD label as ‘depression’, ‘anxiety’, borderline personality disorder, anorexia, and so on. In fact, the distinction between thought and emotion may not even be recognised (Cromby, 2015) and the very notion of an individual who exists in some sense independently from their social network may be alien.” (2018, p. 69-70)
“From a PTM Framework perspective, the trauma-informed model has much to offer. It also has risks and limitations, including: Conceptualising the approach as an alternative explanation for ‘schizophrenia’, ‘bipolar disorder’, ‘ADHD’ and so on, perhaps by reducing adversities to the status of a ‘trigger’ and thus retaining diagnostic categories and thinking . . .” (2018, p.276)
I apologise for the length of the quotes. I’m trying to give you an accurate picture by including some context.
Returning to my story: I revisited the Twitter row, partly because I was angry and looking for a fight and partly because I couldn’t believe that professionals still believed this kind of stuff in 2018.
I’m going to pause now and give myself a pat on the back, as once advised by a psychotherapist.
Despite being angry and upset, I managed to stay calm and polite, except for a couple of little jabs & swipes, as I asked questions and gave feedback to the authors, and yes the medication also helped even when my questions were evaded and ignored. I did, however, get replies from a registered psychologist, supporter of the Framework, who told me, via tweets, that ADHD diagnoses are invalid and damaging. I also saw a tweet from one of the Framework authors in which she stated, “IMO all DX are BS & giving psychoactive meds to kids is immoral. To view ADHD as valid DX seems remarkably lacking in critical thinking.” I’ve kept copies of these tweets.
Eventually, I realised I was wasting my time and energy, the authors didn’t want to hear, even questioned whether I’d read the framework, and then said it was up to me how I used the Framework, I didn’t give the obvious reply! Instead I decided to leave.
I was sorry though to leave behind some of the people I’d met (I’m using the word figuratively) . Not all psychologists support the framework, and the same goes for my fellow service users. In fact the people I met were kind, caring and open-minded, and some even had a wicked sense of humour and mischief. I laughed out loud several times.
I also met service users from the other side of the argument who were kind and helped me to understand and accept their very valid reasons for disliking diagnoses. But my experiences with the professional supporters of the Framework had a completely different nature. I’m not going to give details, it’s not fair. And anyway, we’ve reached the point at which I return to the description I gave earlier of the publication details of the DCP’s position statement and the PTMFramework. My reasons for giving you those dull details at the beginning.
You see, I couldn’t just walk away telling myself that the fuss would die down in a few days and be forgotten. The reality is that the BPS allowed the PTMFramework, despite its evident bias and stigmatising attitude, to be published and available on their website. Registered clinical psychologists promoted it on Twitter, and the BPS and DPC logos are displayed on its front cover. And all this means the PTMFramework carries a backstory of reputability, reliability, and safety. This apparent endorsement by the BPS will encourage the stigmatisation of people with ADHD.
That’s why, here at AADD-UK, we talked and made a plan the first step of which was to send an open letter (below) to the British Psychological Society in which we set out our requests. If these are met we will consider the matter closed as far as we are concerned.
We sent our letter, via Twitter, to BPS on Tuesday, 23rd January but to date we’ve not had a reply.
Never mind, the longer the delay, the longer the length of rope.
We will wait until end of day on Friday, 2 February for a reply.
Transcript of letter sent to BPS as a warning shot across their bows:
Tuesday, 23rd January 2018
Open letter to the British Psychological Society
Re: The Power Threat Meaning Framework (PTMFramework) *
We are a service user organisation and via public promotion on Twitter by the authors and their supporters we were alerted to the open availability of the PTMFramework.
We read it and were shocked by the strong, stigmatising suggestion that ADHD is an illusory, unprofessional, unscientific and unethical diagnosis.
We joined the public Twitter debate & gave this feedback to the lead author as well to @BPSOfficial and @UKDCP. We also pointed out that our views were not sought before publication. We asked for your response.
None has been forthcoming regarding our feedback about these two matters although a registered psychologist, supporter of the framework, did send us inappropriate tweets.
As this has taken place on Twitter, we are using the same platform to ask that the current version of the PTMFramework be retracted to allow the removal of all specific references to ADHD as well as all assertions and/or suggestions that ADHD is an invalid diagnosis.
We also respectfully suggest that the Framework be amended to meet academic standards.
Finally, we ask that you issue a public apology acknowledging the distress and stigmatisation that ADHD service users are experiencing due to the open-access publication and ongoing public promotion of the current version. We suggest that you also respond regarding the unprofessional tweets from the registered psychologist.
If these requests are met, we will consider these specific matters closed as far as we are concerned.
Kind regards,
Susan Dunn Morua on behalf of AADD-UK
@AADDUK (other contact details supplied upon request)
Notes:
1.Many psychologists are NOT supportive of this framework. Additionally, there are service users who reject their diagnosis, for valid reasons, and thus support the framework. AADD-UK fully understands, accepts and supports their right to make this choice. Our letter is only addressing the stigmatising attitude displayed towards ADHD people who have benefited from a psychiatric diagnosis
2. The British Psychological Society is a registered charity which according the blurb on their website does the following:
“. . . acts as the representative body for psychology and psychologists in the UK, and is responsible for the promotion of excellence and ethical practice in the science, education, and application of the discipline.”
And:
“As a society we support and enhance the development and application of psychology for the greater public good, setting high standards for research, education, and knowledge, and disseminating our knowledge to increase the wider public awareness of psychology and its importance.”
References:
Awenat, F. & Berger, M., Coles, S., et al. (2013). Classification of behaviour and experience in relation to functional psychiatric diagnoses: Time for a paradigm shift. DCP Position Statement. Leicester: British Psychological Society
*Johnstone, L. & Boyle, M. with Cromby, J., Dillon, J., Harper, D., Kinderman, P., Longden, E., Pilgrim, D. & Read, J. (2018). The Power Threat Meaning Framework: Towards the identification of patterns in emotional distress, unusual experiences and troubled or troubling behaviour, as an alternative to functional psychiatric diagnosis. Leicester: British Psychological Society
Standards of Conduct, Performance and ethics for registered psychologists
Map of Adult ADHD Services
The Children and Adolescents with ADHD in Transition between Children’s Services and adult Services (CATCh-uS) project team at the University of Exeter ran a survey in 2016 with the aim of creating a map of existing NHS adult ADHD services in the UK, and then they ran another survey at the beginning of this year.
Responses to the 2016 survey have been used to create a preliminary map of existing NHS, voluntary and private services for adults with ADHD whilst the findings from the 2018 survey will be available later this year.
This map not only helps inform and improve services for young people transitioning from child and adolescent mental health services to adult mental health services, it also helps adults who need to access ADHD services. Importantly, the map also highlights areas in the UK where there are gaps in service provision.
Background
CATCh-uS is a very important research study of young people with ADHD in transition from children’s services to adult services. It aims to establish how many young people with ADHD are in need of services for ADHD as adults, and investigate young peoples, parents and practitioners views about the transition process. It is also mapping currently available adult ADHD services around the country. It is funded by the National Institute of Health Research and has been approved by NRES South Yorkshire Ethics Committee – Yorkshire & The Humber (REC Reference: 15/YH/0426) and the University of Exeter Medical School Ethics Committee (REC Application Number: 15/07/070). This study has been adopted by the new HRA on 15th June 2016 (“HRA Approval for a study with an existing UK study wide review”). More details are available on the CATCh-uS website.
How To Deal With Those Tiresome “ADHD” Malingerers by Dr Ivor Schweinekopf
[Editor’s note: Please be aware that this is satire so should not be read by anyone without a sense of humour. And probably not doctors of the old-fashioned sort. Despite this being humorous, all the excuses and maltreatment are based on real situations we have been made aware of, mostly on multiple occasions. Now read on…]
We’ve all had them in our surgeries.
“Oo Doctor, I think I may have ADHD. I’ve got all the symptoms” they whine, as if they know anything about themselves, their minds or medicine. You’ve probably rolled your eyes reading this and nodded in recognition and thought “If only there was a way to get rid of these timewasters!” Or Attention-seeking Dithering Hypochondriac Dolts, I call them.
Well, I’m here to tell you that there is a way. In fact several ways. Let’s have a look at some of them.
A) Ignore them. Yes, you read correctly, ignore them. Change the subject, ask a diverting question, bring up a topic spoken of earlier, or bring up another topic you hadn’t yet got to but had down to mention. Or even better, just come up with something new to worry them. You know what these idiots are like. Change the subject or give them something else to think about and you know they’ll forget what they were talking about until long after you’ve ushered them out of the surgery. Small note here – as you shove them out, point out that there are more patients waiting and you have to be fair to them. Remind your ADHDolt that you are very important and your time is precious, but they aren’t and their time isn’t.
Now you may worry that this tactic might be seen as wilful negligence, but remember that these blithering buffoons probably won’t remember and also really lack legal credibility. Who is going to believe a wittering serial user of mental health services compared to an upright member of the medical profession? No one, that’s who.
B) Deny, deny, deny. Okay, so you’ve got an ADHDolt that actually managed to stay on topic for more than two sentences, what do you do? This is actually more than one tactic, it is several but using the same method. Let’s look at the sub topics: Deny there is such a thing as ADHD in adults. You are important, your ADHDolt is not. Whatever they have read or cited (or brought in in those annoying little print-outs they do), just tell them they are wrong, and the information is wrong. Tell of them the courses and exams you passed and the years of experience you’ve had, and that you can assure them there is no such thing. If you have the nerve, just bluntly tell them you read an article about it in a newspaper and it said there’d no such thing. Start with a paper such as The Times, but you’ll find, as your experience and confidence grows that you can work your way down to The Daily Mail and The Mirror and they’ll accept it. Tip: try not to even sound positive that it exists in children, let alone adults.
- Deny that the NHS treats adult ADHD. Here’s a tip – try to blame it all on Americans. This is a great tactic as it sort of hints you are blaming it on “Big Pharma” without saying it specifically and endangering your relationship with the drug company rep. Also it sort of blames their system (the fact that the actual science is universal and properly conducted research applies the world over is something to avoid) and says how wonderful we (i.e. you are). Tell them that it isn’t really recognised and/or treated in the UK.
- Deny that your area treats ADHD in adults. If they keep whining, agree that some people over here think there might be ADHD in adults but serious people don’t. Of course, if other, slightly odd, people think there’s such a thing as adult ADHD that doesn’t affect your area where people are sensible and don’t believe in such nonsense and your ADHDolt should shut up and stop wasting your time! Tip: For heaven’s sake, don’t let slip you can refer them out of area. And another tip: even if you do have a service in area or a contract with another provider DON’T TELL THEM!
- Deny that they could possibly have it. Of course, officially only a qualified specialists can diagnose ADHD, so, by the same token, only they can (officially) say that someone doesn’t have it. But you are the gatekeeper to those specialists. Don’t open the gates. Tell them they couldn’t possibly have it because of some small success in their life, even if everything else is a disaster. “But you passed GCSE whatever / A level whatever / got into university / have a job / had a job / look smart / have got your shoes on the right way round”. Any and all of these will do.
- Deny all knowledge of anything. In other words, if all else fails, just plead ignorance. That’s it – just claim you don’t know anything about the subject or who or where to refer them. They’re all such a bunch of arses they’ll never work it out for themselves.
If you do have to admit something, only acknowledge their problem long enough to get rid of them, not long enough to make them feel supported, and certainly not long enough to start any treatment. You should say something like: “I feel your pain. I understand your problems. I acknowledge the difficulties you have. Now piss off.”
C) Use delaying tactics. Even if they do work out who or where to be referred (which is pretty hard for a regular patient, let alone one of these disorganised bozos) – sometimes they’ve been along to one of these egregious “self-help groups” (which must be veritable buffoon-fests!”) or managed to print something off www.aadduk.org – a web site created and maintained by what one can only imagine is one of the world’s greatest slag heaps of tosspots and ne’er-do-wells – and they’ve actually got hold of the NICE guidelines and the name of somewhere/someone to be referred to (and, if out of area, a copy of the rules pointing out you are duty bound to refer there if there’s nothing suitable locally), delay!
Tell them you’ll think about it, or that you’ll look into it, to get them out of your office. Then do nothing. Most won’t remember. A good trick that has worked for a lot of people is to simply agree with them (yes, agree!). Tell them you’ll refer them. Then do nothing.
Here’s a great example of tactics I have to take my hat off to. A woman was worried about having ADHD and sought an assessment. Her children and husband all had (and still have) varying degrees and combinations of ADHD and Autism Spectrum Disorder. She was referred to the local service but didn’t hear anything for a while. Three times she followed it up and each time was told she’d hear something within two weeks. Needless to say, each deadline sailed by without her hearing a dickybird. She went to one of these loathsome busybodies that try and help and advocate for such people. The busybody complained and the practitioner was able to come back with not only a bunch of the usual excuses (someone’s on holiday etc etc) but also an absolute blinder. People being assessed for ADHD should chase up their own cases because… wait for it… it empowers them! Genius! Make it difficult for them, ignore them, sideline them and it is good for them! It’s part of the treatment! The sods should be grateful. Punch them in the face and then tell them they should thank you. Masterful use of delaying tactics there, followed up with an assertion so utterly outrageous it is almost impossible to counter. Full marks to whoever thought that one up.
Another brilliant delaying tactic is to find some other problem they’ve got and use that to avoid treating the ADHD. People who have had lifelong ADHD almost always have had anxiety and depression because of it. Just say that you have to treat the depression and anxiety first. Of course, if they go on bogging up their lives because of the ADHD they’ll go on feeling depressed and anxious, so you never have to treat the ADHD!
Quite a few have co-morbid Autism Spectrum Disorder. Get them on that. If any have mood swings or anger management problems, and they show them on front of you (or even a member of staff), you can bung them out on the spot for being abusive, and anyway you can put down “difficult patient” in their file’s private bit.You may even be able to get them banned from almost all the primary medical services in the whole area.
Or put them down as having a personality disorder (there are several, take you pick). A lot of areas don’t treat personality disorders so that finishes that, but even if your area does have such a service, and you actually think the patient does have a personality disorder, just treat them for that alone. Don’t make the mistake of admitting that it is possible to have ADHD and something else at the same time.
If you didn’t want to see people with mobility problems, you could agree to only see them in an office that is up three flights of stairs with no lift. Do the psychological equivalent to the ADHDolts. They just don’t have the gumption or organisation to stick at anything so just keep giving them hoops to jump through.
D) Divert. If denying or delaying doesn’t work, divert. Send them to the wrong type of therapy – in particular to a therapist that knows little of ADHD. This is widely practiced. One good example we know of was someone who had an assessment saying “Emma doesn’t have ADHD because she can concentrate sometimes.” [Editor’s note: if you don’t know why this is nonsense, then you really don’t understand ADHD. Name changed, BTW.]
Only a psychiatrist can diagnose ADHD so make sure to send patients to anything but a psychiatrist. Then, even if the person does realise the patient has ADHD, there is nothing they can do about it. That works so often, and even now never fails to make me laugh!
E) Discontinue. But, just suppose they’ve previously been treated by one of the increasing number of modern goody-goody doctors (who are letting the side down quite frankly). Suppose they actually are getting some treatment (thankfully probably only medication on a long-term basis) all is not lost. Get them off it!
There are all sorts of excuses, sorry, I mean reasons. Age is a good one. Almost every complaint treated is treated for the whole of the patient’s life, but sometimes they’ll believe the age thing with ADHD.
Keep doing blood tests. Liver ones are good, but do as many as you can. You might not take someone off statins at the first sign of liver problems, but do so with ADHD meds.
If any one of the possible side effects even if unlikely occur (and there’s a huge list on the leaflet with the medication – as with any medicine the leaflet has to list even the really unlikely and unproven ones), take them off. Now arguably you are supposed to refer them to an expert, but hey, just stop the prescription and let the ADHDolt argue. To see a specialist they have to go through you!
Depression and anxiety are great excuses. In one list of possible but unlikely side effects is “Behaving With Excessive Cheerfulness And Activity”! A happy productive member of society? We can’t have that. Get them off the stuff at once!
Oh, and any possible addiction or substance abuse even if you only have circumstantial evidence is a great excuse to get them off the meds. Now a lot of these whiners say they sometimes have trouble remembering to take their medication, which on the face of it looks rather the opposite of addiction. Have you ever heard an alky exclaim, “Damn, I forgot to drink vodka today!”? But remember, what you feel about the matter is a much better guide than what the patient reports.
F) And finally, if all else fails, remember to stigmatise them. The poor little darlings, because of their ‘life difficulties’ become sensitive to rejection. (Let’s be honest, if they didn’t keep claiming they had anything wrong with them, they wouldn’t keep getting rejected!) Be patronising. Ask them if they get a buzz off the meds. Tell them they are lucky to be seen at all, let alone diagnosed. Tell them how controversial the whole topic is, how expensive the drugs are, that they aren’t trying hard enough (especially on timekeeping – even if your surgery habitually runs late). After all, shame has been shown to work so well with topics such as addiction and obesity, and, let’s be honest, and the GUM clinics are a disgrace the way they go around treating people for diseases in a non-judgemental way. Let’s hope it doesn’t spread to the rest of the medical field or well end up letting these ADHDolts off the hook for their moral failings!
Goodbye and Don’t Forget To Grind The Bastards Down!
Ivor Schweinekopf
[Editor’s note: We would be delighted to hear your personal experience of trying to get assessed or treated for ADHD in the UK – we may be able to do a follow-up article. Please contact the (real) author: theunreadyaethelred@gmail.com
If you have or might have ADHD or otherwise been affected by this article please come to an ADHD support group or join our forum, and if you are having trouble getting treatment Here’s the relevant page on NICE, and here’s a summary of your rights and here are some more – try printing them out and taking them with you (sorry, currently in England, other regions to follow), and of course, please tell your story be it gruesome or funny – they’re often both – to Aethelred The Unready who is currently saddling his horse to sally forth against the ranking hordes of Schweinekopfs.]
We welcome your sharing this on social media and elsewhere, please give attribution to (the real) author and site.
This work is licensed under the Creative Commons Attribution-ShareAlike 4.0 International License. To view a copy of this license, visit http://creativecommons.org/licenses/by-sa/4.0/.
It was originally published here.

Bridging the gap: optimising transition from child to adult mental healthcare
The following has been taken from the introduction to an Expert Policy Paper that explores the reasons why transitioning from child to adult mental healthcare is problematic and challenging. We’ve put a link to the full paper at the end of the following introduction:
Transition to adult services is often a difficult time for young people living with a mental
health condition. The journey through adolescence into adulthood is a time of significant
physical, psychological and social change not only for the adolescent, but also their
families. Overall rates of mental health problems can also increase during adolescence and issues become more complex, and in some cases serious disorders such as psychosis
may emerge. During this period, adolescents may also have a greater tendency for risky
behaviour, become lost in the system between child and adult mental health services and are also at greater risk of disengagement from services.
This Expert Policy Paper was developed on the basis of an Expert Working Meeting on
Mental Health and Transition, held in Brussels on 11 July 2017. The meeting brought
together expert clinicians (psychiatrists and neurologists), patient representatives, academics and mental health advocacy groups to explore the reasons why transition of care is currently suboptimal, discuss and agree on the principles for good transition and develop practical recommendations for improving transition to adult mental healthcare services. The group included expert stakeholders from the field of transition of care, mental health in general and attention-deficit hyperactivity disorder (ADHD).
The Expert Working Group highlighted that the problems associated with transition from child to adult services are not disease-specific; they apply to all mental health disorders, for example, epilepsy, autism and social phobia. However, to identify practical policy solutions, the Expert Working Meeting focused on ADHD as a case study in the analysis of the problems, barriers to change and potential solutions associated with transition of care.
ADHD is a diverse condition characterised by symptoms of inattention, hyperactivity
and impulsivity that can have a significant impact on patients’ lives. ADHD is relatively
common and often persists into adulthood. Despite this, access to adult ADHD services
and support is generally poor, resulting in frequent gaps in care.2,11 For these reasons,
ADHD provides an example in which to frame transition to adult services across the
mental health sector.
If you would like to read the full Policy Paper, please click on Bridging the Gap
Clinical Guideline (CG72) ADHD: diagnosis & management Update
NICE Guidelines are recommendations for the treatment and care of people with ADHD by health professionals within the NHS. They are based on the best available research evidence and their aim is to improve the quality of healthcare. The guidelines are also used to develop standards to assess the clinical practice of ADHD clinics and services and are used in the education and training of health professionals. They also help us, people with ADHD, to make informed decisions and improve communication between us and the health professionals. When a guideline is developed, organisations can register as stakeholders (AADD-UK is a registered stakeholder) which means that they are consulted throughout the development process.
The original guidelines (on the diagnosis and management of ADHD) were published in September 2008 and are now being updated. The update covers the areas of identification of risk factors, post diagnostic advice, non-pharmacological and pharmacological management and intervention adherence for children, young people and adults with a diagnosis of ADHD. It does not cover any other aspect from the previous guideline.
The consultation period started on the 6th September 2017 and will end on 18th October 2017 at 5 pm. The updated guidelines are expected to be published on 21st February 2018.
NICE accepts comments during the consultation period from organisations that are registered as stakeholders but individuals can submit comments by contacting the stakeholder organisation that most closely represents their interests. AADD-UK is a stakeholder organisation and will be submitting comments so if you would like to add your suggestions or comments please feel free to send them to us by email at aadd.org@gmail.com. Here is a link to the NICE website with more information about the ADHD Guideline update.
ADHD: Surviving or Thriving?
Here at AADD-UK we avidly followed the news about mental health issues during Mental Health Awareness Week. We admired the bravery of those telling their own stories, we retweeted some general mental health links instead of those that only dealt directly with ADHD, all the while preparing for our 10th Year Anniversary by revamping our website. Then suddenly we realised we’d forgotten the elephant in our own parlour! So we decided to write, just before the week ended, our own position for Mental Health Awareness Week.. Here it is:
First, we thanked the Mental Health Foundation for hosting the week, and thanked them for commissioning the survey and consequent report “Surviving or Thriving? The state of the UK’s mental health.” The authors of the report wrote that despite “many areas of advances in human health we are not seeing these reflected in mental health. If anything, the signs are that we are slipping back.” They backed this up by shockingly disclosing that only 13% of those surveyed in England, Scotland and Wales had “high positive mental health” and that nearly “two-thirds of people say that they have experienced a mental health problem” and others were clearly “just about surviving.”
The authors further reported that those of us living with either low household incomes or unemployment have worse mental health than those employed at higher incomes. 3 in 4 people at the lowest income level, 85% of unemployed people, 7 in every 10 women, 7 in every 10 young adults (aged 18-34), and 7 in 10 people living alone experienced poor mental health. Additionally, the authors quoted the “Mental Health and Wellbeing in England: Adult Psychiatric Morbidity Survey 2014” (published last year) which revealed that every week 1 in 6 adults experienced a “common mental health problem, such as anxiety or depression. 1 in 5 adults reported that they had considered taking their own life at some point.”
I sat in silence and reflected upon those numbers and felt an overwhelming sadness. So much unnoticed desperation and despair! Swiftly followed by anger; “Who can I blame?” “Where shall I point my finger?” You see, all this correlated almost exactly with our own experiences in the ADHD world.
It’s been almost 10 years since we set up AADD-UK with hope and optimism. During that 10 years, the National Institute for Health and Clinical Excellence (NICE) published ADHD Guidelines in which adults were included for the first time. Of course there was some initial resistance but over the years more and more professionals became interested, more and more moved into the field, more and more research confirmed ADHD as valid (even the usual tabloid suspects now, tentatively, report positive ADHD stories) and there are more ADHD services in the UK than the 3 that existed 10 years ago.
But all is not well! As awareness of ADHD grows, funding for ADHD services dwindles. Some GP’s, due to funding shortages, are reluctant to refer us to services. In truth, not all of the ADHD services have enough funding to meet the NICE Guidelines. It’s even been suggested, in one known circumstance, that the Guidelines be disregarded. A couple of services have surreptitiously tried to close. Some have decided not to publicise their contact details for fear they’ll get more referrals than allowed for by their funding. Of course, this means that waiting lists are getting longer and longer; even up to 2 years long! It’s true that gate keepers and sign posters cheerily point us to psychological therapies suggesting we use them while waiting. But guess what? Yep that’s right! We’re shuffled onto the end of another waiting list where some of us must try not to listen to whispers about the low quality of the offerings. So, there we are, stuck waiting, struggling to cope with abysmally low self-esteem, hurting, lonely, barely surviving. What does this matter when it’s said that ADHD makes us resilient, that we’re used to hard knocks, that we’re survivors? It matters because we understand too well that surviving is not thriving and that knowledge is painful!
And what about those of us who’ve been diagnosed and are taking medication? We’re all thriving right? Well not exactly. Medication is indeed all that some of us need. We can now concentrate as well as focus better. That helps us to, at last, move on and up. It helps us to feel relief as well as feel the joy of achievement. Some of us can even choose between seeing a consultant privately for follow-ups or waiting months to see the same consultant on the NHS. There’s a group of us too who, after a competent diagnosis of ADHD, don’t need any further help, not even medication. It’s enough that somebody listened, took us seriously, evaluated patterns underlying our difficulties, and found a way to help us understand. That’s all we needed to find our own way, to thrive and flourish.
Some of us, though, have been so pressured and battered by an uncomprehending and stigmatising life that the clarity that comes with medication also carries the aching revelation that our graceful childhood spirits have turned into cut-down and subjugated ghosts. Taking the right medication is not all we need. Before we can move from surviving to thriving we need help, we need to rediscover our true spirits, our real potential. Yet we’re stuck in the low income, or underemployed, or unemployed bracket. So we ask the NHS for help, get sign posted to psychological therapies, by the same cheery folk our clan members encountered, and off we shuffle to join the end of a waiting list. There we are waiting, masks firmly in place (we don’t want pity), acting as if we don’t care but feeling worn-out, inside crying, mourning for our lost and trusting childhood. We’re surviving and that’s all!
Still, at least the mere fact that we’re waiting allows us a bit more hope than those of us who’ve not been noticed. Some of us in this group are being shuffled from one wrong diagnosis to another wrong diagnosis, from one wrong medicine to another wrong medicine. Never having our true reality heard or acknowledged. Some of us become disheartened, lose faith and sink into helplessness. And then what about those of us who learn to believe from early on that we are seemingly born to live life as a failure, never understanding why that appears to be our fate? All of us too are barely surviving!
It’s such a waste because every single one of us with ADHD has the potential to flourish. We would love to use our strengths and abilities to help others, to be a benefit. We don’t need much. Just the right attention and the right support at the right time. Actually you know what? That’s not hard to provide!
Now I’m angry again so I’m jumping right off the fence and pointing my finger squarely at you, the Government. I’m pointing at you, Theresa May, as well as at you, Jeremy Hunt. If you get back in charge, for goodness sake stop with your wasteful changing, privatising and building inequality into the health service. Instead, if you really care about helping people to thrive, helping the country to prosper (you do, don’t you?), stand back and for once look at the big picture.
The prevalence rate for children with ADHD is between 5 to 7%, of whom approximately 65% will continue to experience symptoms in adulthood. In other words, roughly 3% to 4% of all adults have ADHD. To make it clearer, about 1 in 25 adults have ADHD. That’s a lot of us! That’s a lot of us costing you a lot of money!
Leaving us unrecognised, undiagnosed, untreated or treated ineffectively, or pushing us onto waiting lists is costing you, the Government, a lot of money in lost tax revenue, inappropriate treatments, repeat visits to A&E, clearing up after our accidents, looking after our brothers and sisters in prisons, and so on and so on (you want evidence, ask and we’ll give it freely). It’s cheaper, far cheaper, to increase NHS mental health funding so that all of us can receive proper help! We want to use our strengths, abilities and skills. We can use them to thrive and flourish!
And here’s a final note, the need for mental health awareness and funding did not disappear with the end of Mental Health Awareness Week. The two thirds of people living in England, Scotland and Wales who’ve experienced mental health problems, including all of us with ADHD, are still here on Monday morning. Funding and treatment for everybody experiencing mental ill health is still needed and is still vital. With that, and with preventative care, all of us will thrive and flourish and so too will the country.
I’ve had my say for now! It’s time for you, the Government (whichever of you ends up in charge) to listen and act!
BBC Horizon Documentary
BBC Horizon is making a documentary exploring ADHD. There will be two strands to the documentary and so they are looking for two groups of contributors with experiences with ADHD as follows:
Call out #1
“Does your child have ADHD?
BBC Horizon is making a documentary exploring ADHD, aiming to create a wider public understanding of the condition. Presented by Rory Bremner, a comedian with a particular interest in ADHD, the BBC is hoping to shed light on this commonly misunderstood condition.
The BBC wants to meet parents of children with ADHD who can tell them about what life’s like; and to also hear from their child about their own experience of the condition.
If you’re interested, please get in touch with Zoe on zoe.huntergordon@bbc.co.uk, just for a chat in the first instance. The BBC will be very pleased to hear your story.
Call out #2
“Do you have ADHD? Do you feel it has it impacted your life?
BBC Horizon is making a documentary exploring ADHD, looking at the variety of ways that mild to severe ADHD can impact people’s lives in both a negative and or even positive way: with the aim of to increasing public understanding of this condition. It will be presented by Rory Bremner, a comedian who has first-hand experience of the condition. For a specific item of the programme, we want to hear from people with ADHD who feel their condition might have contributed to them entering the criminal justice system.
Please do get in touch if you think this is you. In the first instance, it would just be a chat on the phone – you do not need to commit to anything upfront.
The BBC appreciates the sensitive nature of the subject, and will handle all calls with the utmost confidentiality and respect.
The BBC is interested by the fact that ADHD is overrepresented in the prison population, and are interested in speaking with people who feel as though their ADHD may have contributed to their criminal behaviour. They hope that by sharing your story, the BBC can help to shed light on this commonly misunderstood disorder.
If you’re interested, please get in touch with Zoe on zoe.huntergordon@bbc.co.uk: just for a chat in the first instance.”
UKAAN Conference: ADHD in the Mainstream
The UK Adult ADHD Network (UKAAN) will host its 6th Congress from Wed 20th to Fri 22nd September 2017. This 3 day conference will take place at the Mermaid Conference and Events Centre, which will accommodate up to 600 delegates in a Theatre. The venue is situated between the City and the West End, on the North Bank of the Thames, and enjoys spectacular views towards the Tate Modern, Globe Theatre and the Millennium Bridge.
The conference is titled ‘ADHD in the mainstream’ to reflect the rapid increase in recognition and treatment of ADHD by adult mental health services. ADHD is a common disorder effecting around 5% of children and 3% of adults, with symptoms and impairments that overlap with other common mental health disorders. The role that ADHD plays in the health of many adults presenting with mental health problems is now much more widely recognised, yet recent evidence suggests that in many cases the disorder still goes unrecognised or treated. Our vision is to bring ADHD into the mainstream, so that all mental health professionals have the knowledge and understanding to diagnose and treat ADHD, in the same way as other common mental health disorders.
This meeting aims to raise the level of awareness, knowledge and expertise among health care professionals about people with ADHD and provide a better understanding of the persistence of the disorder, the development of comorbid mental health problems and the delivery of effective treatments.
The program will be delivered by prominent opinion leaders, clinical experts and internationally recognised investigators and is designed to cover key topics relevant to the diagnosis and treatment of ADHD from adolescence to early and late adulthood. The selection of speakers is particularly important so that the audience can hear directly from the most experienced professionals working in this rapidly developing area of clinical psychiatry.
Registration is now open on the UKAAN Website http://www.ukaan.org/adhd-in-the-mainstream/
The CATCh-uS ADHD Survey is now live
Please help us with a study from the University of Exeter. The project is about children and young people with Attention Deficit Hyperactivity Disorder in transition between children’s services and adult services.
One piece of the project, however, is a mapping survey designed to find out which adult ADHD services are out there for young people with ADHD aged 18 and over to transition into from children’s services. This means that this survey can be answered by any person of any age who has knowledge of ADHD services, whether they have ADHD themselves or not and whether they are a parent/carer or not.
If you click on this link https://www.surveymonkey.co.uk/r/CATCh-uS_SU you will be guided to a page where you can tell the researchers about adult ADHD services in your area – or equally important the lack of adult services. The online questionnaire asks no more than 8 questions and should take less than 5 minutes to complete.
The survey is anonymous and your response will contribute to the creation of a map detailing adult ADHD services currently available in the UK. If you want more information about the project, the research team have a website where you can find more information: http://medicine.exeter.ac.uk/catchus/mapping/
Thank you very much for helping us with this project.
Complaint to Chief Whip re Mr Graham Allen MP & ADHD ‘not a real disease’
Update on 2nd May 2014: to email sent to the Opposition Chief Whip regarding Graham Allen MP and his guest Dr Bruce Perry of “ADHD not a real disease” infamy.
I have not yet had a reply to the letter below which I sent on Tuesday, 8th April 2014 despite the fact that I was told by a member of Rosie Winterton’s staff that we would get a reply within two weeks.
I was polite and gave them three weeks to allow for the Easter week, and then rang Rosie Winterton’s office yesterday morning (Thursday, 1 May 2014) at 9:15 am. An equally polite chap answered the phone, he recognised the name of AADD-UK and he knew about our complaint. He explained that the Special Advisors (Spads) were “looking at it” and would get back to us. I asked which Spad in particular is “looking at” the complaint, and if he had any idea when the Spad would get back to us. The polite chappie said he didn’t know when we would get an answer because he’s just the civil servant, but he did give me the name of the Spad, Luke Sullivan. The civil servant also told me that he’d again put our complaint in front of Luke Sullivan.
Fingers crossed this is more promising than it sounds! Somehow the “Thick of It” popped into my mind during this conversation.
Just as a BTW I see that Luke Sullivan was a Spad in the Chief Whip’s office when Gordon Brown was Prime Minister (2009) which surprised me because I thought Spads got sacked when their bosses left. The document I looked at also gave his pay scale which wasn’t bad, not bad at all considering that he was only in pay band 2 which was near the bottom.
And just in case you are wondering who Rosie Winterton is, well she was Labour’s pension minister when The Telegraph wrote about her on 29th May 2009 in relation to the expenses scandal. And if you read the article (click here) you will see that her salary wasn’t bad, not bad at all, and much, much better than Luke’s.
Now I’m going to confess to you that before I rang Rosie Winterton’s office I had an ADHD moment and by mistake I rang the office of the Parliamentary Commissioner for Standards (that’s the office that found Maria Miller MP guilty of claiming £45,000 in expenses to which she wasn’t entitled, and was then subsequently overruled by a committee of MP’s–beg their pardons there were three lay members on the committee except of course they weren’t allowed to vote).
After we’d sorted out that I wasn’t talking to the person I thought I was, we had a nice chat about how members of the public can hold MP’s accountable for their conduct (after I’d explained that we’d already written to Ed Miliband, Harriet Harman, Rosie Winterton, and of course Mr Graham Allen himself and were still waiting to hear from any of them) and as a result of our little chat I’ve now learnt that as members of the public we’ve got 3 options namely vote next year (duh!!), get legal advice (expensive waste of money when we already know Graham Allen is wrong,) or go to the media (aha!).
So there we are for the moment; waiting to hear something (hopefully more than nothing)from Mr Luke Sullivan, SpAd to Opposition Chief Whip, Rosie Winterton MP Labour. We’ll keep you updated!
Further Update: 2nd May 2014 p.m.
And now we read in the Closer that Katie Hopkins (the former apprentice that Sir Alan Sugar called unemployable) has made it her mission to attack mothers of children with ADHD. Even worse according to today’s article in the Closer, Katie Hopkins was “inspired into ‘badmouthing’ ADHD children by Dr Bruce Perry” and what’s more the remainder of the article contains several unhelpful remarks about ADHD that were made by Katie’s ‘hero’ on the eve of his visit to the UK. Dr Perry was invited to the UK by Graham Allen MP. So thank you very much Mr Allen for encouraging the likes of Katie Hopkins!
Tuesday, 8th April 2014
The following email has been sent from AADD-UK to the Opposition Chief Whip:
Right Honourable Ms Rosie Winterton, Opposition Chief Whip
I am writing on behalf of Adult Attention Deficit Disorder – UK (AADD-UK) to make a complaint about Mr Graham Allen. We have tried to resolve the matter directly with Mr Allen but he has not responded.
Mr Allen has endorsed an article that appeared in the Observer on Sunday, 30th March 2014 titled “ADHD ‘not a real disease’ says US neuroscientist.” Mr Allen has placed a photograph of this article (30th March) on his official Twitter account (@GrahamAllenMP) along with the caption “Dr Bruce Perry, my Early Intervention hero, in UK today, want to attend his EIF events over next 2 days?”
In addition, Mr Allen also has placed a photograph on Twitter (1st April) which is captioned “Dr Bruce Perry speaks to Labour shadow ministers this morning”, this photograph and caption gives the appearance that Dr Perry’s views could potentially also be the Labour Party’s views (I have attached copies of Mr Allen’s Tweets).
We feel that Mr Allen is potentially in breach of the Code of Conduct for Members of Parliament namely:
1. Members have a duty to uphold the law, including the general law against discrimination.
We feel that it is harassment for a public figure, an MP, to invite and host a doctor who in the past has spoken against ADHD, and then to publicly approve his guest’s stigmatising opinion made on the eve of his visit to the UK that ADHD is not real. It is harassment not only because ADHD is a recognised disability that meets the requirements for a protected characteristic under the Equality Act 2010, but also because people with ADHD in the UK already had significant problems with daily living intensified by shame generated from home-grown discriminatory comments and behaviour. We did not, therefore, need Members of Parliament validating such derogatory opinions and thus causing us further humiliation and distress.
2. Members have a general duty to act in the interests of the nation as a whole; and a special duty to their constituents.
Given that the prevalence rate for ADHD in the UK is between 2-5%, it is more than likely that Mr Allen has constituents with ADHD. His inviting and hosting a guest such as Dr Perry who openly speaks his mind about ADHD, followed by Mr Allen’s public endorsement of Dr Perry’s views makes it nearly impossible for Mr Allen’s constituents who either have ADHD themselves, or care for someone with ADHD, or have a friend or relation with ADHD to contact him and ask him to represent their interests and concerns in the House of Commons. It also means that they are excluded from political activities for as long as Mr Allen remains their MP.
The National Institute of Clinical Excellence, in 2008, completed a full review of the diagnosis and treatment of ADHD across the lifespan and published guidelines in September 2008. These guidelines did help to stimulate the development of service provision for ADHD in the UK. But ADHD services, particularly for adults, are still too scarce in the UK. This is of relevance for children and young people because as they transition from Child and Adolescent Mental Health Services there are frequently no adult services available in their area. And unfortunately austerity measures have meant that many mental health services have been cut, and sometimes waiting lists for ADHD services can be as long as 18 months! Indeed sometimes the barriers are so high that people with ADHD have resorted to asking their MP’s for help accessing services. This makes it all the more disappointing that Mr Allen presents himself as endorsing the view that ADHD is not real, because this means that people will be deterred from going to their MP’s for help, not just for ADHD matters but for any reason.
Mr Allen is not setting a good example and this is not good for the nation because the proportion of people receiving treatment for ADHD in the UK is lower than the prevalence rate and failure to treat ADHD is costly to society. There is plenty of evidence to show that untreated ADHD leads to increased rates of unemployment, addictions, criminal convictions, and poor social adjustments. I have included links to relevant documents at the end of this email.
In addition, when Mr Allen endorsed Dr Perry’s opinions in a Tweet and followed this up with a Tweet accompanied by a photograph of Labour Shadow Ministers listening to Dr Perry, and a photograph of Dr Perry with Francis Maude the perception was created that it could be Labour policy as well as Coalition Government Policy to discount ADHD as a valid disorder. That’s a deterrent that would inhibit the rest of us from also engaging with the entire political process.
3. Members should act on all occasions in accordance with the public trust placed in them. They should always behave with probity and integrity, including in their use of public resources.
Dr Perry would possibly not have had a chance to express his opinions in the UK media if he had not been invited to come and meet Government ministers by Mr Allen. But he was invited here, and his opinions have been endorsed and validated by Mr Allen, not just by the publication of the photograph that we described earlier, but by the fact that Mr Allen helped Dr Perry meet with Government officials including Iain Duncan Smith, Jeremy Hunt, and Francis Maude (see attached photograph) and also with Labour Shadow Ministers. This creates the further perception, rightly or wrongly, that taxpayer money is being used to help promote anti-ADHD views, as well as to pay for the time of ministers and others who met with Dr Perry, who sat and listened to his presentations, and who in at least one case was photographed with him.
4. “Members shall base their conduct on a consideration of the public interest, avoid conflict between personal interest and the public interest and resolve any conflict between the two, at once, and in favour of the public interest.” (V, 10)
We most definitely feel that Mr Allen has confused and mixed his personal interests and opinions with public interests regarding his work in early intervention, his reports about early intervention, as well as his creation of the Early Intervention Foundation. We are concerned that Mr Allen invited, hosted, and endorsed Dr Perry who on the eve of his visit to the UK to meet with Government ministers on behalf of Early Intervention expressed to a major newspaper the biased and inflammatory opinion that ADHD is not real because that makes us wonder how Mr Allen’s Early Intervention Foundation will be able to provide “practical advice and support to those trying to make Early Intervention a reality on the ground” when at the core there appears to be a complete lack of knowledge and acceptance that a common neurological disorder affecting behaviour and attention is indeed real.
To resolve this conflict in favour of public interest we feel that ADHD should always be a consideration in anything relating to early intervention whether it be of Mr Allen’s design or that of others, and we would like written assurance regarding that. We should also like Mr Allen to withdraw all photographs and references relating to Dr Perry from his Tweets and that includes the photograph of the Observer article. And finally we would like a letter of apology from Mr Allen which we will publish.
At the bottom of this email is a sampling of some of the articles that appeared in the traditional press repeating response to Dr Perry’s opinions (Dr Perry was also widely quoted in many other news sources, various blogs, forums, Facebook, and Twitter), as well as a sampling of information about ADHD.
I look forward to hearing from you.
Dr Bruce Perry: ADHD is “not a real disease”
AADD-UK has sent the following email to Graham Allen MP with copies to Ed Miliband, Harriet Harman, & Andy Burnham:
Dear Mr Allen,
I am very sorry to say this but one of your tweets (at 12:46 p.m. on Sunday, 30 Mar 2014) has caused considerable offence. It is a photograph of a newspaper article entitled “ADHD ‘not a real disease’ says US neuroscientist” and above it you have placed the following caption: “Dr Bruce Perry, my Early Intervention hero, in UK today . . .”.
I have attached a copy of your tweet.
The offence caused by the photograph is made worse by your use of the word “hero” to describe Dr Perry.
Also, I don’t know if Dr Perry was misquoted in the Observer, but if he wasn’t it was not helpful for your guest to make such statements about ADHD (an area in which he does not have specialised knowledge) on the eve of his visit to the UK. His remarks, as stated in The Observer, were very widely publicised in many reputable and otherwise newspapers, blogs, and forums. And all this at a time when people with ADHD are already struggling to overcome considerable stigma and discrimination as well as struggling to access much needed help so that they can live fulfilled lives. The firestorm of adverse publicity increased the distress and anxiety of many people with ADHD.
Would you please consider taking down the offending tweet and offering an apology to people with ADHD. I appreciate that you are trying to do your best for children through the Early Intervention Foundation, but since mental health services (and other much needed services) have been badly affected by the coalition government’s cuts, we all, adults included, need at least some politicians that we feel will listen.
I look forward to hearing from you.
So now we are waiting to see if they are listening! We’ll keep you updated!
ADHD – Mind, Brain and Body
The UK Adult ADHD Network (UKAAN) will host its 4th Congress in September 2014, entitled ADHD – Mind, Brain and Body, in conjunction with ENAA and APSARD. The conference will take place over 3 days, at the Mermaid Conference and Events Centre which is situated between the City and the West End in London. Located on the North Bank of the Thames, it enjoys spectacular views towards the Tate Modern, the Globe theatre and the Millennium Bridge. The theatre will accommodate 600 people, and there will also be opportunities to attend parallel sessions throughout the event.
The conference will bring together internationally recognised experts in the diagnosis and treatment of ADHD across the lifespan and highlight basic science and clinical research that contributes to our current understanding of ADHD as a lifespan disorder. Clinical services for ADHD during the transition years from adolescence to adulthood and for those newly diagnosed as adults are developing rapidly throughout many parts of Europe. The conference will build on this growing expertise by providing a uniquely European perspective that highlights the full range of functional, cognitive and mental health impairments, the impact that ADHD has on adolescent and adult mental health and the contribution to adolescent and adult psychopathology. This meeting will address important clinical and scientific questions relating to ADHD and will be relevant to anyone interested in the mental health of people from the adolescent years through to early, middle and later adult life.
This meeting aims to raise the level of awareness and knowledge among health care professionals about people with ADHD as they grow older; and to provide a better understanding of the causal pathways involved in the persistence of the disorder and the development of important clinical comorbidities. The program will be delivered by prominent opinion leaders, clinical experts and internationally recognised investigators and is designed to cover key topics relevant to the diagnosis and treatment of ADHD during the critical period from adolescence to adulthood. The selection of speakers is particular important so that the audience can hear directly from the most experienced professionals working in this rapidly developing area of clinical psychiatry.
The UK Adult ADHD Network (UKAAN) was established in March 2009 to provide support, education, research and training for mental health professionals working with adults with Attention Deficit Hyperactivity Disorder (ADHD). UKAAN was founded by a group of experienced mental health specialists who run clinical services for adults with ADHD within the National Health Service.
More information about the 4th Congress, and registration details are available on UKAAN’s website here.
UKAP – Reducing the costs of ADHD Across Education, Health and Care
UKAP (the UK ADHD Partnership) will host its first conference on Friday 4th April 2014. This one day event will take place at the Thistle Charing Cross Hotel, London, with a conference on ‘Reducing the Costs of ADHD across Education, Health and Care’ .
The aim of the meeting is to introduce, education, healthcare and allied professionals to the UKAP committee’s objective to raise the profile of ADHD on the political agenda in order that young people with ADHD gain better recognition and access to treatment across educational, occupational, youth justice and healthcare settings.
UKAP would also like to invite parents, carers other voluntary sector organisations and support groups who are working to support ADHD, to join them in their call to action which seeks to inform policy makers and authorities of the importance of early identification and intervention.
With presentations on the costs of ADHD, the impact on education, the family, the youth justice system, health service, accidental injury and driving, UKAP will consider what can be done to reduce the burden of ADHD on children, the family and more broadly in society. The programme will include presentations by prominent opinion leaders, and internationally recognised clinical and educational practitioners.
This meeting will be relevant to all education and healthcare practitioners working with children and young people, together with allied professionals involved in multi-agency working including educational, occupational and youth justice settings, as well as commissioners and policy makers.
For more information and registration details see the UKAP website here.
Close to an Act: how did the Health and Social Care Bill get passed?
AADD-UK has received permission from Mike Birtwistle, Head of MHP Health, to reproduce his analysis as to how the Health and Social Care Bill is now set to become an Act, barring any last-minute dramatic revelations. We asked for Mike’s permission because his analysis helps us to understand how these reforms might impact our access to assessments, diagnosis, and treatment for ADHD, and also helps us to figure out how we can address impacts resulting from these reforms.
Close to an Act: how did the Health and Social Care Bill get passed?
Submitted by Mike Birtwistle on 20-03-2012
It’s all over, bar some (more) shouting. The Health and Social Care Bill is nearly law but, after hundreds of hours of debate, thousands of amendments and countless controversies, what will it actually mean? And how on earth did it ever get passed?
Theoretically the Queen could decline to give Royal Assent to the Bill, as Unite suggested last week. However, barring any constitutional outrages or last minute shocks in the Commons, it will become an Act. And the Health and Social Care Act will represent one of the longest and most complex items of health legislation ever known. That it passed through a hung Parliament, in the teeth of such controversy is no small feat.
For better or worse, the Act will represent one of the most profound pieces of reforming legislation ever (alongside the Attlee reforms of the 1940s and some of the market reforms of the last Conservative Government). I believe all three sets of reforms have problems, but the scope of their impact and ambition is undeniable. Continue reading
ADHD: Transition from Adolescence to Adulthood
The UK Adult ADHD Network (UKAAN) will hold the 3rd Congress on the 29th June 2012. The theme will be ‘Transition of ADHD from Adolescence to Adulthood’. The conference will be located in Central London at Savoy Place, 2 Savoy Place, City of London WC2R 0BL
The congress aims to bring important topics on transition in ADHD to a wider audience. The scientific program will include five main sessions, with a panel and audience discussion
Clinical services for ADHD during the transition years from adolescence to adulthood and for those newly diagnosed as adults are developing rapidly. This meeting will address important clinical and scientific questions relating to ADHD and will be relevant to anyone interested in the mental health of people from the adolescent years through to early, middle and later adult life.
For more information and registration details for this important conference please go to the UKAAN website.
Get Involved in a New Government Disability Strategy
Brighton Adult ADHD Group has been invited to contribute directly to a new cross-government disability strategy. The Government has published a discussion document with questions and Brighton Adult ADHD Group wants to gather your views, to make sure we represent the experiences of people with ADHD in Sussex.
To share your views please come to our discussion event. We will have a speaker from the Office for Disability Issues.
Date: Wednesday 7th March
Time: 18.30 – 20.00
Location: The Brunswick Room, The Brighthelm Centre, North Road, Brighton, BN1 1YD
Light refreshments will be provided
For further information please contact Caroline Williams on 01403 733931
We want to talk about practical ideas that will make a real difference to your life. The Government has asked us to focus on three areas:
- realising aspirations
- increasing individual control
- changing attitudes and behaviours
We have made a questionnaire with questions relating to each area that can be downloaded here. It would be helpful if you could fill in your responses before coming to the meeting, and bring them with you. If you are unable to attend the meeting, please email your responses as soon as possible to mail@adhdbrighton.org.uk
We will send a report of our event to the Government. They will look at everyone’s suggestions and work with disabled people to publish a new strategy later this year.
If you want to find out more visit www.odi.gov.uk/fulfillingpotential
Update:Cambridgeshire’s denial of NHS treatment for adults newly diagnosed with ADHD
AADD-UK has not yet received an official response to our letter (see previous post on this subject) regarding the actions taken by NHS Trusts and Commissioning Groups in Cambridgeshire which restrict access to NICE recommended treatments for people who are diagnosed as adults with ADHD. However, we notice that the new low priority policy for ADHD has been removed from the website for the Cambridgeshire and Peterborough Public Health Network and has been replaced by the words “Please note this policy has been temporarily withdrawn.” You can read this for yourself here.
Now we do realise that this removal could just be coincidence, and may or may not be a good sign. But Cambridgeshire County Council, who also received a copy of our letter, has made a very positive move. The Council’s “Adults Wellbeing and Health Overview and Scrutiny Committee” has listed under Agenda Item 7a (for their meeting on 8 February 2012) in “Committee priorities and work programme 2011/12” the following: “Provision of medication for adults with ADHD: The Chairman has received representations from individuals with ADHD on this issue. It is proposed that the Chairman and Vice-Chairman, with the support of the Scrutiny and Improvement Officer, follows this up with NHS Cambridgeshire.”
Well done and a big AADD-UK Thank You to Councillor Kevin Reynold, the Chairman of the Committee!
The meeting of the Adults Wellbeing and Health Overview and Scrutiny Committee is open to the public so if you live in Cambridgeshire and have been affected by the low priority policy do please go to the meeting. The meeting is on Wednesday 8 February 2012 at 2:30 PM in the Kreis Viersen Room, Shire Hall, Cambridge. More details are available on their website here.
And again, Thank You Councillor Reynold!

You must be logged in to post a comment.